Toh Sengwee, Hampp Christian, Reichman Marsha E, Graham David J, Balakrishnan Suchitra, Pucino Frank, Hamilton Jack, Lendle Samuel, Iyer Aarthi, Rucker Malcolm, Pimentel Madelyn, Nathwani Neesha, Griffin Marie R, Brown Nancy J, Fireman Bruce H
Ann Intern Med. 2016 Jun 7;164(11):705-14. doi: 10.7326/M15-2568. Epub 2016 Apr 26.
Recent postmarketing trials produced conflicting results about the risk for hospitalized heart failure (hHF) associated with dipeptidyl peptidase-4 (DPP-4) inhibitors, creating uncertainty about the safety of these antihyperglycemic agents.
To examine the associations of hHF with saxagliptin and sitagliptin.
Population-based, retrospective, new-user cohort study.
18 health insurance and health system data partners in the U.S. Food and Drug Administration's Mini-Sentinel program.
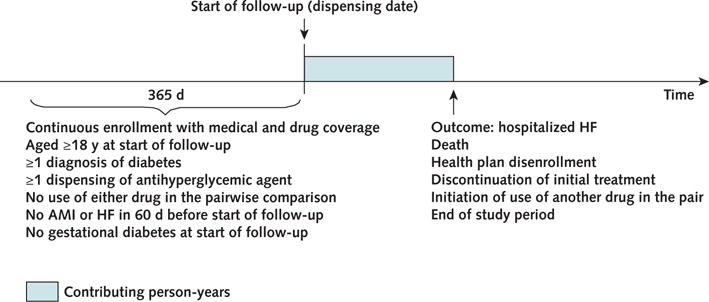
Patients aged 18 years or older with type 2 diabetes who initiated therapy with saxagliptin, sitagliptin, pioglitazone, second-generation sulfonylureas, or long-acting insulin products from 2006 to 2013.
Hospitalized HF, identified by International Classification of Diseases, Ninth Revision, Clinical Modification codes 402.x1, 404.x1, 404.x3, and 428.xx recorded as the principal discharge diagnosis.
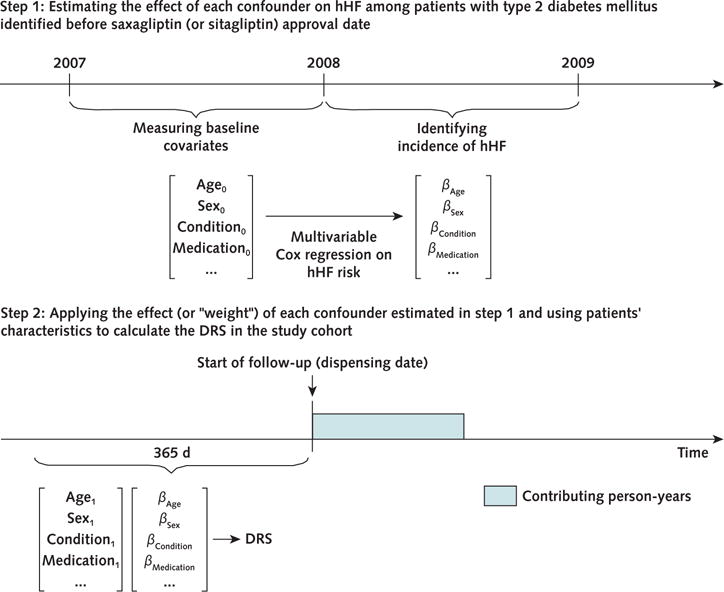
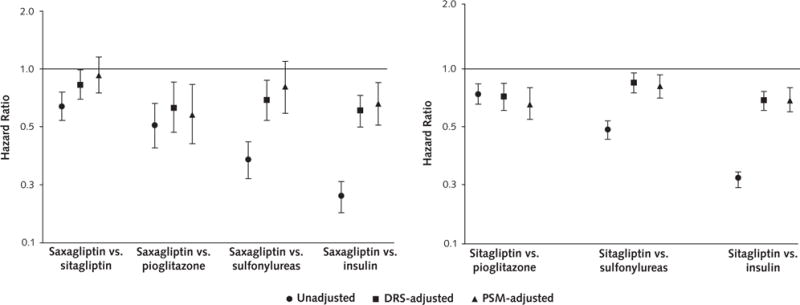
78 553 saxagliptin users and 298 124 sitagliptin users contributed an average of 7 to 9 months of follow-up data to 1 or more pairwise comparisons. The risk for hHF was not higher with DPP-4 inhibitors than with the other study drugs. The hazard ratios from the disease risk score (DRS)-stratified analyses were 0.83 (95% CI, 0.70 to 0.99) for saxagliptin versus sitagliptin, 0.63 (CI, 0.47 to 0.85) for saxagliptin versus pioglitazone, 0.69 (CI, 0.54 to 0.87) for saxagliptin versus sulfonylureas, and 0.61 (CI, 0.50 to 0.73) for saxagliptin versus insulin. The DRS-stratified hazard ratios were 0.74 (CI, 0.64 to 0.85) for sitagliptin versus pioglitazone, 0.86 (CI, 0.77 to 0.95) for sitagliptin versus sulfonylureas, and 0.71 (CI, 0.64 to 0.78) for sitagliptin versus insulin. Results from the 1:1 propensity score-matched analyses were similar. Results were also similar in subgroups of patients with and without prior cardiovascular disease and in a subgroup defined by the 2 highest DRS deciles.
Residual confounding and short follow-up.
In this large cohort study, a higher risk for hHF was not observed in users of saxagliptin or sitagliptin compared with other selected antihyperglycemic agents.
U.S. Food and Drug Administration.
近期的上市后试验对于二肽基肽酶 - 4(DPP - 4)抑制剂相关的住院心力衰竭(hHF)风险产生了相互矛盾的结果,这使得这些降糖药物的安全性存在不确定性。
研究hHF与沙格列汀和西他列汀之间的关联。
基于人群的回顾性新用户队列研究。
美国食品药品监督管理局微型哨点计划中的18个医疗保险和卫生系统数据合作伙伴。
2006年至2013年开始使用沙格列汀、西他列汀、吡格列酮、第二代磺脲类药物或长效胰岛素产品进行治疗的18岁及以上2型糖尿病患者。
通过国际疾病分类第九版临床修订本编码402.x1、404.x1、404.x3和428.xx记录为主要出院诊断的住院心力衰竭。
78553名沙格列汀使用者和298124名西他列汀使用者为1次或多次成对比较贡献了平均7至9个月的随访数据。DPP - 4抑制剂导致hHF的风险并不高于其他研究药物。疾病风险评分(DRS)分层分析得出的风险比为:沙格列汀与西他列汀相比为0.83(95%CI,0.70至0.99);沙格列汀与吡格列酮相比为0.63(CI,0.47至0.85);沙格列汀与磺脲类药物相比为0.69(CI,0.54至0.87);沙格列汀与胰岛素相比为0.61(CI,0.50至0.73)。DRS分层风险比为:西他列汀与吡格列酮相比为0.74(CI,0.64至0.85);西他列汀与磺脲类药物相比为0.86(CI,0.77至0.95);西他列汀与胰岛素相比为0.71(CI,0.64至0.78)。1:1倾向评分匹配分析的结果相似。在有和没有既往心血管疾病的患者亚组以及由DRS最高的两个十分位数定义的亚组中结果也相似。
残余混杂因素和随访时间短。
在这项大型队列研究中,与其他选定的降糖药物相比,未观察到沙格列汀或西他列汀使用者发生hHF的风险更高。
美国食品药品监督管理局。