Kraszewska-Głomba Barbara, Szymańska-Toczek Zofia, Szenborn Leszek
Wrocław Medical University.
Bosn J Basic Med Sci. 2016 Mar 10;16(2):157-61. doi: 10.17305/bjbms.2016.974.
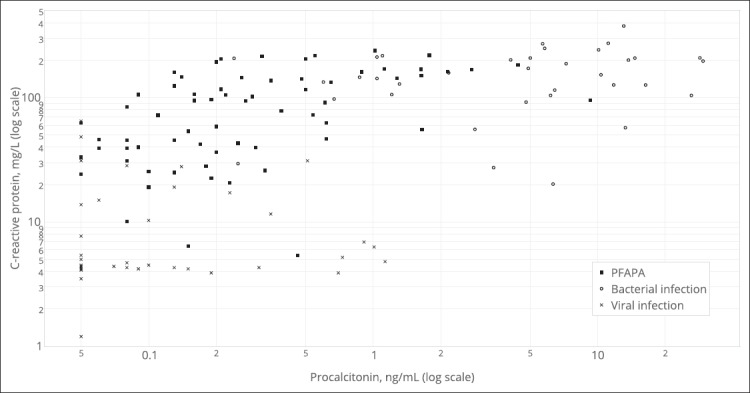
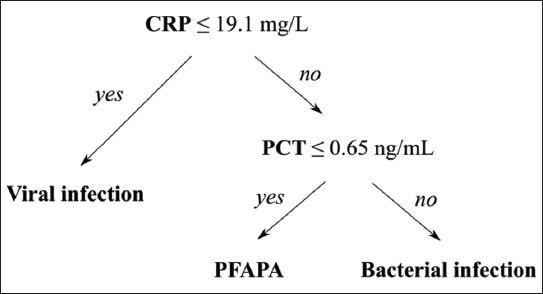
As no specific laboratory test has been identified, PFAPA (periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis) remains a diagnosis of exclusion. We searched for a practical use of procalcitonin (PCT) and C-reactive protein (CRP) in distinguishing PFAPA attacks from acute bacterial and viral infections. Levels of PCT and CRP were measured in 38 patients with PFAPA and 81 children diagnosed with an acute bacterial (n=42) or viral (n=39) infection. Statistical analysis with the use of the C4.5 algorithm resulted in the following decision tree: viral infection if CRP≤19.1 mg/L; otherwise for cases with CRP>19.1 mg/L: bacterial infection if PCT>0.65ng/mL, PFAPA if PCT≤0.65 ng/mL. The model was tested using a 10-fold cross validation and in an independent test cohort (n=30), the rule's overall accuracy was 76.4% and 90% respectively. Although limited by a small sample size, the obtained decision tree might present a potential diagnostic tool for distinguishing PFAPA flares from acute infections when interpreted cautiously and with reference to the clinical context.
由于尚未确定特异性实验室检查,周期性发热、口疮性口炎、咽炎和颈淋巴结炎(PFAPA)仍需排除其他疾病后才能诊断。我们探索了降钙素原(PCT)和C反应蛋白(CRP)在区分PFAPA发作与急性细菌和病毒感染方面的实际应用价值。对38例PFAPA患者以及81例诊断为急性细菌感染(n = 42)或病毒感染(n = 39)的儿童测定了PCT和CRP水平。使用C4.5算法进行统计分析得出以下决策树:若CRP≤19.1 mg/L,则为病毒感染;否则对于CRP>19.1 mg/L的病例:若PCT>0.65 ng/mL,则为细菌感染,若PCT≤0.65 ng/mL,则为PFAPA。该模型采用10倍交叉验证进行测试,在一个独立测试队列(n = 30)中,该规则的总体准确率分别为76.4%和90%。尽管受样本量小的限制,但谨慎解读并结合临床情况时,所得决策树可能为区分PFAPA发作与急性感染提供一种潜在的诊断工具。