Pun Shawn C, Plodkowski Andrew, Matasar Matthew J, Lakhman Yulia, Halpenny Darragh F, Gupta Dipti, Moskowitz Chaya, Kim Jiwon, Steingart Richard, Weinsaft Jonathan W
Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY.
Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, NY.
J Am Heart Assoc. 2016 May 4;5(5):e003368. doi: 10.1161/JAHA.116.003368.
Cardiac magnetic resonance (CMR) imaging is well validated for tissue characterization of cardiac masses but has not been applied to study pattern and prognostic implications of cardiac metastases (CMETs) among patients with systemic cancer.
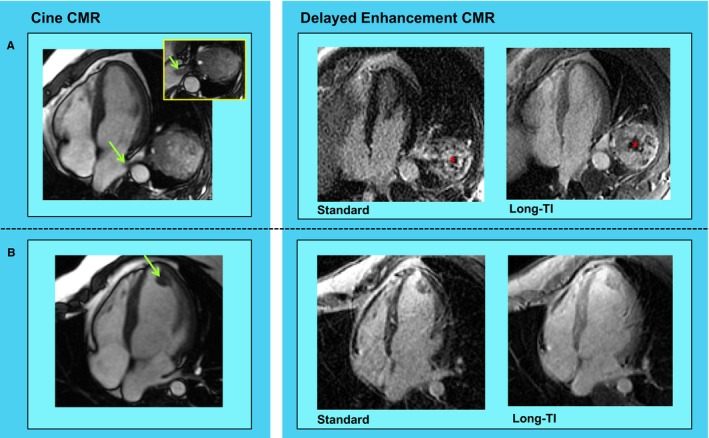
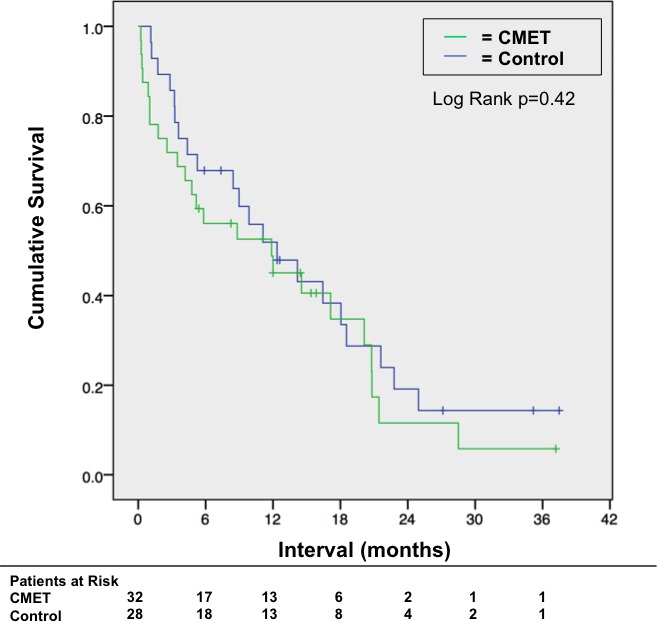
The population consisted of 60 patients with stage IV cancer (32 patients with CMETs, 28 diagnosis-matched controls) undergoing CMR. CMET was defined as a discrete mass with vascular tissue properties on delayed enhancement CMR. CMET-positive patients and controls had similar clinical characteristics, cardiac geometry, and function (P=NS). Leading cancer types associated with CMET were sarcoma, melanoma, and gastrointestinal. Patients with CMETs had similar distribution of extracardiac metastatic disease compared with controls (organs involved: 3.4±2.0 versus 2.7±1.9, P=0.17). In 94% of patients with CMETs, there were metastases involving ≥1 extracardiac organ (66% lung involvement). CMET location varied (right ventricle 44%, right atrium 19%, left ventricle 28%, left atrium 9%, pericardial 25%); 22% of cases had multichamber involvement. Right-sided chamber involvement was common in hematologic/lymphatic spread (67%); pericardial involvement was common with direct spread (64%). Regarding tissue properties on delayed enhancement CMR, CMETs commonly (59%) demonstrated heterogeneous enhancement (41% diffuse enhancement). Heterogeneous lesions were larger and had increased border irregularity (P<0.05). Survival 6 months post-CMR was numerically lower among patients with CMETs (56% [95% CI 39-74%]) versus stage IV cancer-matched controls (68% [95% CI 50-86%]), although differences between groups were nonsignificant (P=0.42).
CMETs vary regarding etiology, location, and tissue properties on CMR, highlighting need for comprehensive surveillance of cardiac involvement regardless of cancer origin. Prognosis remains poor with for patients with CMETs, albeit similar to that for stage IV cancer controls matched for cancer etiology.
心脏磁共振成像(CMR)在心脏肿块的组织特征分析方面已得到充分验证,但尚未应用于研究全身性癌症患者中心脏转移瘤(CMET)的模式及预后影响。
研究人群包括60例接受CMR检查的IV期癌症患者(32例CMET患者,28例诊断匹配的对照)。CMET定义为延迟强化CMR上具有血管组织特性的离散肿块。CMET阳性患者和对照具有相似的临床特征、心脏几何形态和功能(P=无显著性差异)。与CMET相关的主要癌症类型为肉瘤、黑色素瘤和胃肠道肿瘤。与对照相比,CMET患者的心外转移性疾病分布相似(累及器官:3.4±2.0对2.7±1.9,P=0.17)。在94%的CMET患者中,存在累及≥1个心外器官的转移(66%累及肺部)。CMET的位置各不相同(右心室44%,右心房19%,左心室28%,左心房9%,心包25%);22%的病例有多腔室受累。右侧腔室受累在血液学/淋巴系统扩散中常见(67%);心包受累在直接扩散中常见(64%)。关于延迟强化CMR上的组织特性,CMET通常(59%)表现为不均匀强化(41%为弥漫性强化)。不均匀病变更大且边界不规则性增加(P<0.05)。CMR检查后6个月时,CMET患者的生存率在数值上低于IV期癌症匹配对照(56%[95%CI 39-74%]对68%[95%CI 50-86%]),尽管两组间差异无统计学意义(P=0.42)。
CMET在病因、位置和CMR组织特性方面各不相同,突出了无论癌症起源如何都需要对心脏受累进行全面监测的必要性。CMET患者的预后仍然很差,尽管与癌症病因匹配的IV期癌症对照相似。