Huang Yao-Ting, Neofytos Dionysios, Foldi Julia, Kim Seong Jin, Maloy Molly, Chung Dick, Castro-Malaspina Hugo, Giralt Sergio A, Papadopoulos Esperanza, Perales Miguel-Angel, Jakubowski Ann A, Papanicolaou Genovefa A
Infectious Disease Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York.
Infectious Disease Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York; Department of Medicine, Weill Cornell Medical College, New York, New York.
Biol Blood Marrow Transplant. 2016 Aug;22(8):1480-1486. doi: 10.1016/j.bbmt.2016.05.003. Epub 2016 May 10.
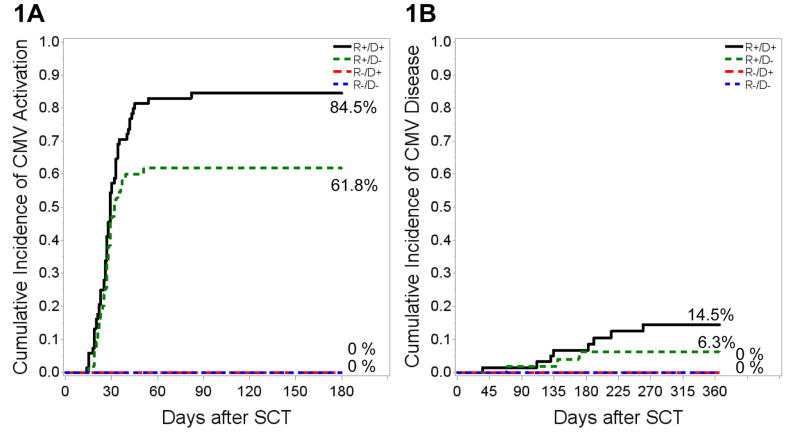
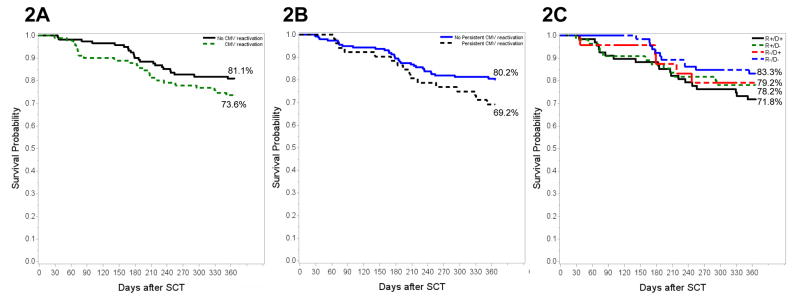
The effectiveness of preemptive treatment (PET) for cytomegalovirus (CMV) in recipients of ex vivo T cell-depleted (TCD) hematopoietic cell transplantation (HCT) by CD34(+) selection is not well defined. We analyzed 213 adults who received TCD-HCT at our institution from June 2010 through May 2014. Patients were monitored by a CMV quantitative PCR assay if recipient (R) or donor (D) were CMV seropositive. CMV viremia occurred early (median, 27 days after HCT) in 91 of 213 (42.7%) patients for a 180-day cumulative incidence of 84.5%, 61.8%, and 0 for R+/D+, R+/D-, and R-/D+ patients, respectively. CMV disease occurred in 5% of patients. In Cox regression analysis, R+/D+ status was associated with increased risk for CMV viremia compared with R+/D- (hazard ratio [HR], 1.79, 95% confidence interval [CI], 1.16 to 2.76, P = .01), whereas matched unrelated donor allograft was associated with decreased risk (HR, .62; 95% CI, .39 to .97, P = .04). Of 91 patients with CMV viremia, 52 (57%) had persistent viremia (>28 days duration). Time lag from detection of CMV viremia to PET was associated with incremental risk for persistent viremia (HR, 1.09; 95% CI, 1.01 to 1.18; P = .03). Overall, 166 of 213 (77.9%) patients were alive 1 year after HCT, with no difference between patients with and without CMV viremia or among the different CMV serostatus pairs (P = not significant). CMV viremia occurred in 70% of R + TCD-HCT. Delay in PET initiation was associated with persistent viremia. With PET, CMV R/D serostatus did not adversely impact survival in TCD-HCT on 1-year survival in the present cohort.
通过CD34(+)选择对体外T细胞去除(TCD)造血细胞移植(HCT)受者进行巨细胞病毒(CMV)抢先治疗(PET)的有效性尚不明确。我们分析了2010年6月至2014年5月在我院接受TCD-HCT的213名成年人。如果受者(R)或供者(D)CMV血清学阳性,则通过CMV定量PCR检测对患者进行监测。213名患者中有91名(42.7%)早期发生CMV病毒血症(中位数,HCT后27天),180天累积发病率分别为84.5%、61.8%和0,分别对应R+/D+、R+/D-和R-/D+患者。5%的患者发生了CMV疾病。在Cox回归分析中,与R+/D-相比,R+/D+状态与CMV病毒血症风险增加相关(风险比[HR],1.79;95%置信区间[CI],1.16至2.76;P = 0.01),而匹配的无关供体同种异体移植与风险降低相关(HR,0.62;95%CI,0.39至0.97;P = 0.04)。在91名发生CMV病毒血症的患者中,52名(57%)存在持续性病毒血症(持续时间>28天)。从检测到CMV病毒血症到进行PET的时间间隔与持续性病毒血症风险增加相关(HR,1.09;95%CI,1.01至1.18;P = 0.03)。总体而言,213名患者中有166名(77.9%)在HCT后1年存活,发生CMV病毒血症的患者与未发生者之间以及不同CMV血清学状态组之间无差异(P = 无显著性)。70%的R + TCD-HCT患者发生了CMV病毒血症。PET开始延迟与持续性病毒血症相关。在本队列中,对于TCD-HCT的1年生存率,PET治疗时CMV R/D血清学状态对生存没有不利影响。