Lin Andrew, Flynn Jessica, DeRespiris Lauren, Figgins Bradley, Griffin Meagan, Lau Carmen, Proli Anthony, Devlin Sean M, Cho Christina, Tamari Roni, Jakubowski Ann A, Papadopoulos Esperanza B, Giralt Sergio A, Perales Miguel-Angel, Seo Susan K, Shaffer Brian
Department of Pharmacy, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, New York.
Transplant Cell Ther. 2021 Jan;27(1):85.e1-85.e6. doi: 10.1016/j.bbmt.2020.10.009. Epub 2020 Oct 11.
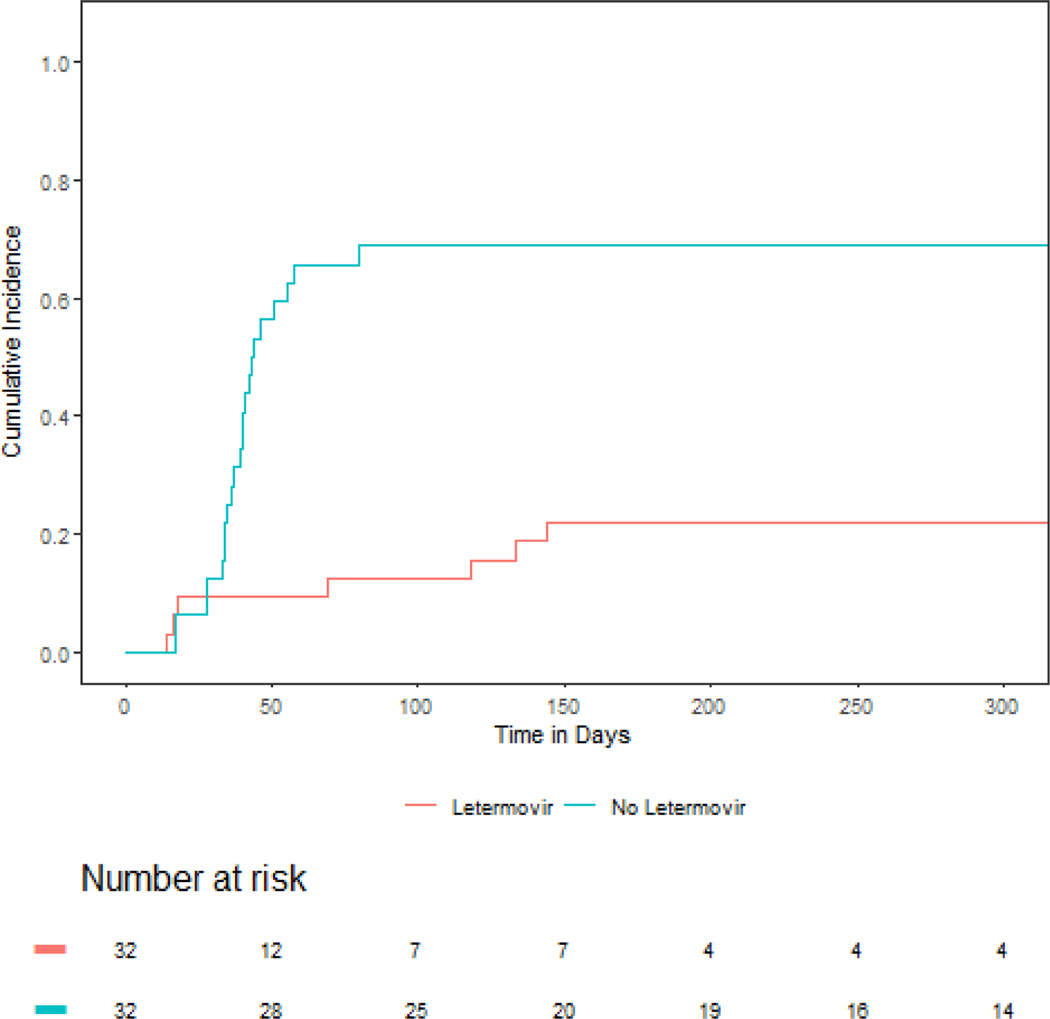
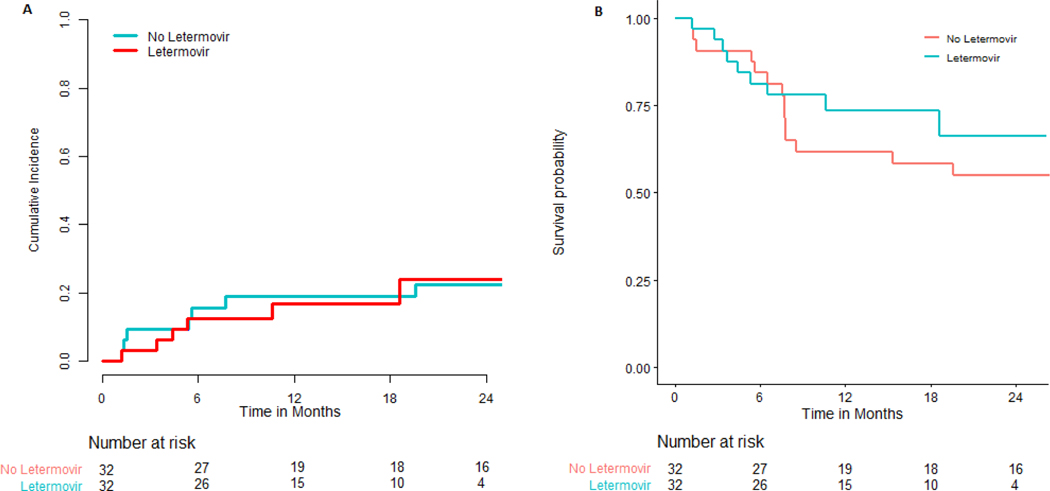
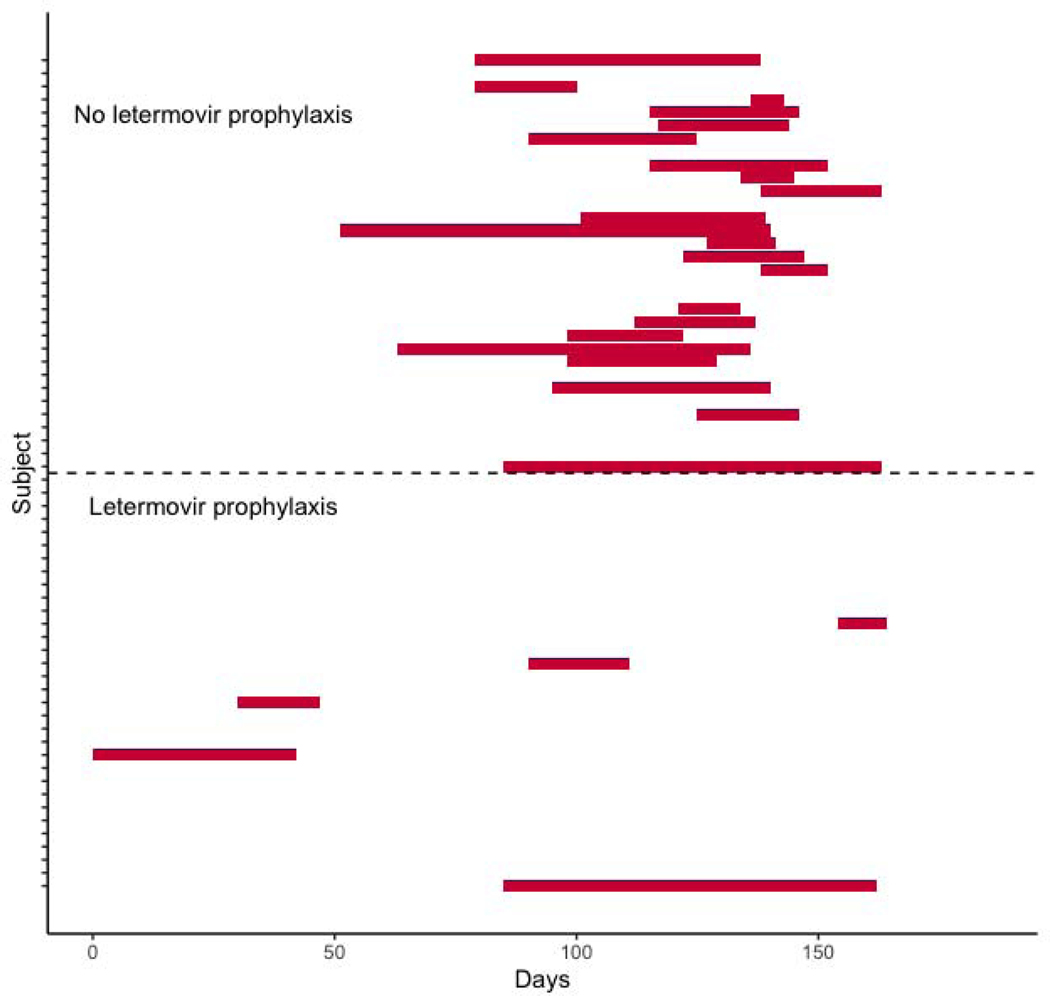
Cytomegalovirus (CMV) is serious viral infection in allogeneic hematopoietic cell transplantation (allo-HCT) recipients. November 2017, the novel CMV DNA terminase complex inhibitor letermovir was approved for prophylaxis of CMV infection in CMV-seropositive allo-HCT recipients. Here we sought to determine the effectiveness of letermovir in preventing CMV infection in CMV-seropositive patients undergoing haploidentical or mismatched adult unrelated donor allo-HCT using post-transplantation cyclophosphamide-based graft-versus host-disease prophylaxis. Sixty-four patients underwent transplantation between 2014 and 2019, of whom 32 received letermovir and 32 did not receive letermovir. The day 180 cumulative incidence of CMV infection requiring therapy was 45.3% (95% confidence interval [CI], 32.7% to 57.1%) in the entire cohort, 68.8% (95% CI, 48.9% to 82.2%) in the patients who did not receive letermovir, and 21.9% (95% CI, 9.5% to 37.6%; P < .001) in patients who received letermovir. Adjusting for regimen intensity, disease histology, and age, the hazard ratio for CMV infection was .19 (95% CI, .08 to .47; P < .001) in patients who received primary prophylaxis with letermovir. The 1-year cumulative incidence of treatment- related mortality was similar between patients with and without letermovir treatment (16.9% versus 18.9%), as was overall survival (64.0% versus 49.0%). Persistent CMV infection requiring >28 days of therapy was more common in patients who did not receive letermovir (31.2% versus 6.2%; P = .02). In summary, letermovir was effective in preventing CMV infection in this high-risk population of HLA-mismatched allo-HCT recipients.
巨细胞病毒(CMV)感染是异基因造血细胞移植(allo-HCT)受者中一种严重的病毒感染。2017年11月,新型CMV DNA 末端酶复合物抑制剂来特莫韦被批准用于预防CMV血清反应阳性的allo-HCT受者的CMV感染。在此,我们试图确定来特莫韦在预防接受单倍体相合或不匹配的成人无关供者allo-HCT且采用基于移植后环磷酰胺的移植物抗宿主病预防方案的CMV血清反应阳性患者的CMV感染方面的有效性。2014年至2019年期间,64例患者接受了移植,其中32例接受了来特莫韦治疗,32例未接受来特莫韦治疗。在整个队列中,需要治疗的CMV感染的180天累积发病率为45.3%(95%置信区间[CI],32.7%至57.1%),未接受来特莫韦治疗的患者中为68.8%(95%CI,48.9%至82.2%),接受来特莫韦治疗的患者中为21.9%(95%CI,9.5%至37.6%;P<.001)。在调整方案强度、疾病组织学和年龄后,接受来特莫韦一级预防的患者发生CMV感染的风险比为0.19(95%CI,0.08至0.47;P<.001)。接受来特莫韦治疗和未接受来特莫韦治疗的患者的1年治疗相关死亡率相似(分别为16.9%和18.9%),总生存率也相似(分别为64.0%和49.0%)。需要治疗>28天的持续性CMV感染在未接受来特莫韦治疗的患者中更为常见(分别为31.2%和6.2%;P = 0.02)。总之,来特莫韦在预防这种高风险的HLA不匹配allo-HCT受者人群的CMV感染方面是有效的。