Brouillette Marie-Josée, Yuen Tracy, Fellows Lesley K, Cysique Lucette A, Heaton Robert K, Mayo Nancy E
Department of Psychiatry, McGill University, McGill University Health Centre, Montreal, Canada.
Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Canada.
PLoS One. 2016 May 18;11(5):e0155766. doi: 10.1371/journal.pone.0155766. eCollection 2016.
While HIV-associated neurocognitive impairment remains common despite the widespread use of combined antiretroviral therapy (cART), there have been relatively few studies investigating the trajectories of neurocognitive change in longitudinal NeuroAIDS studies.
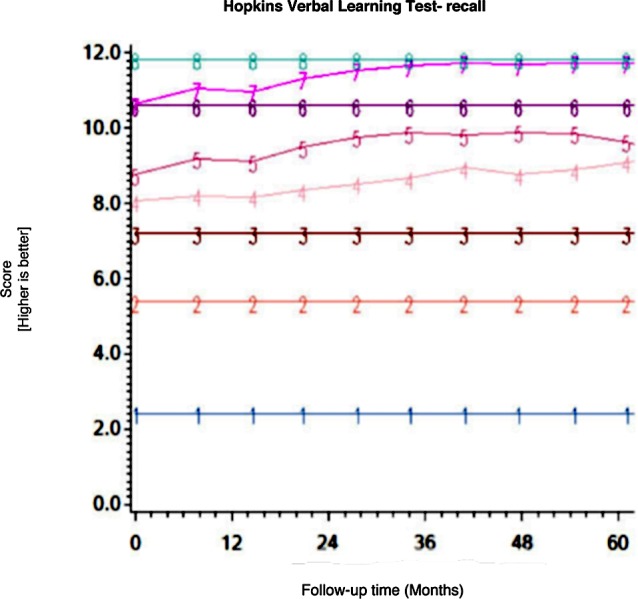
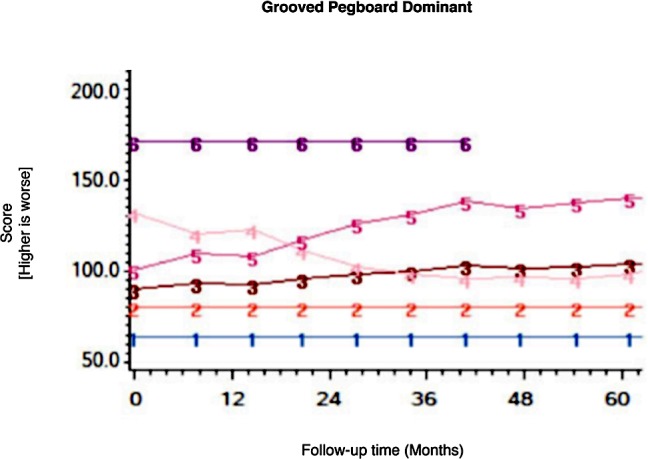
To estimate the magnitude and pattern of neurocognitive change over the first 3 years of follow-up using Group-Based Trajectory Analysis (GBTA) applied to participants in the longitudinal arm of the CHARTER cohort.
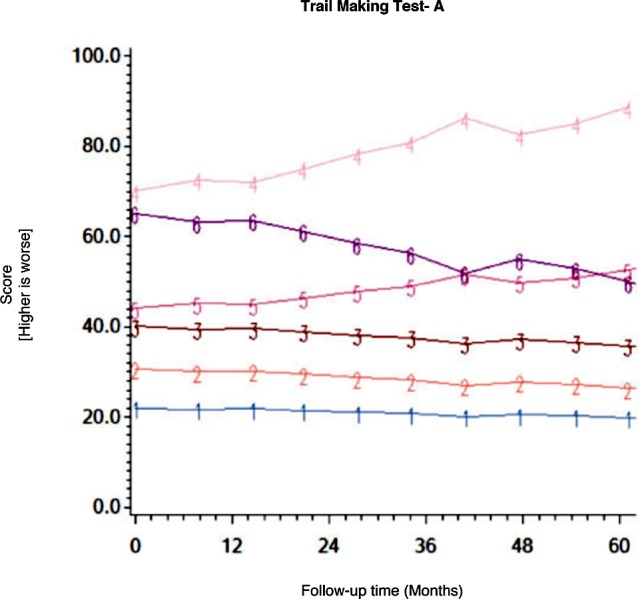
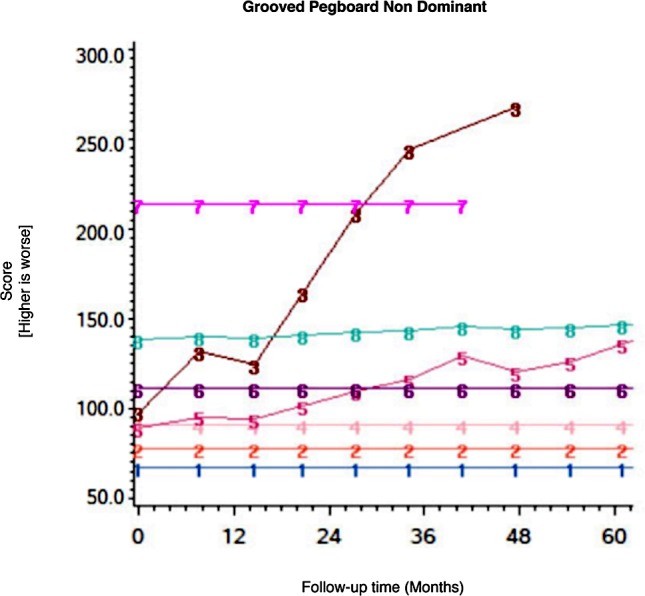
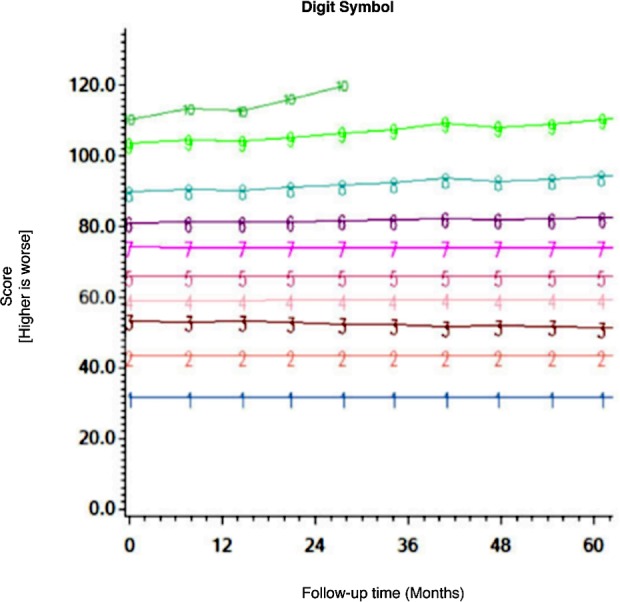
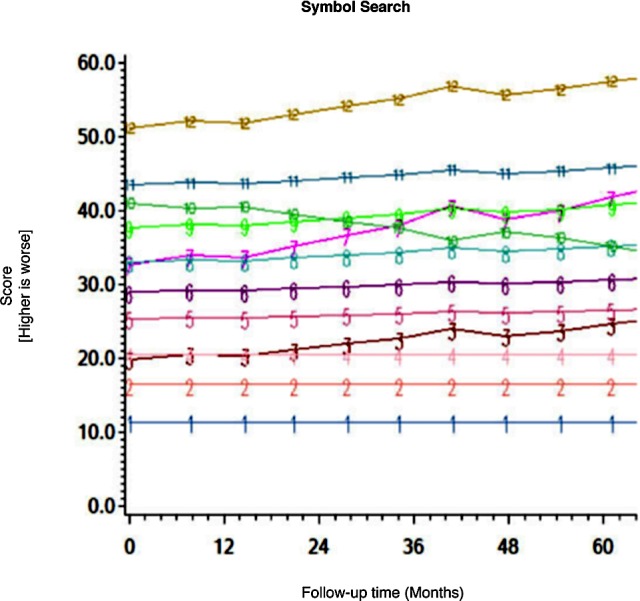
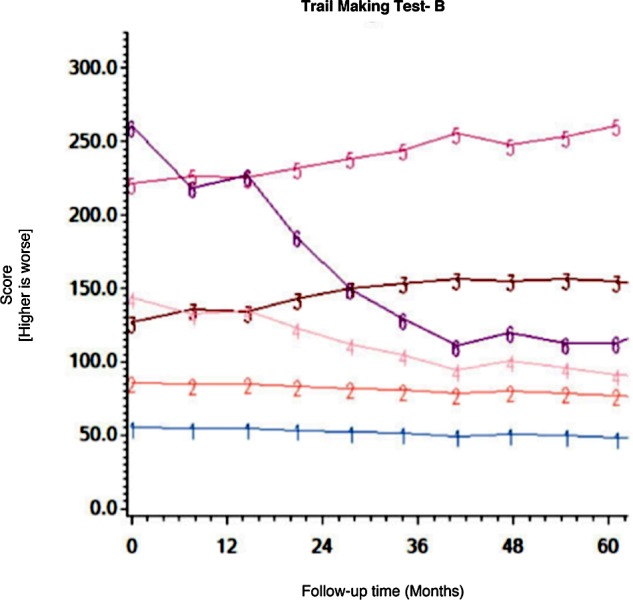
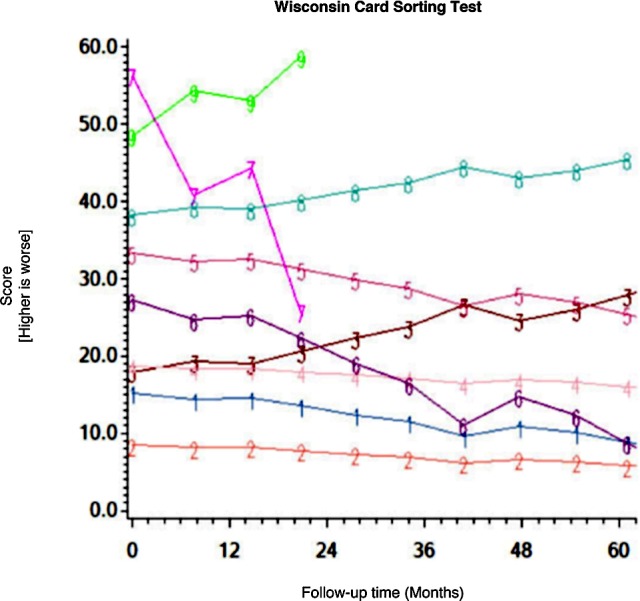
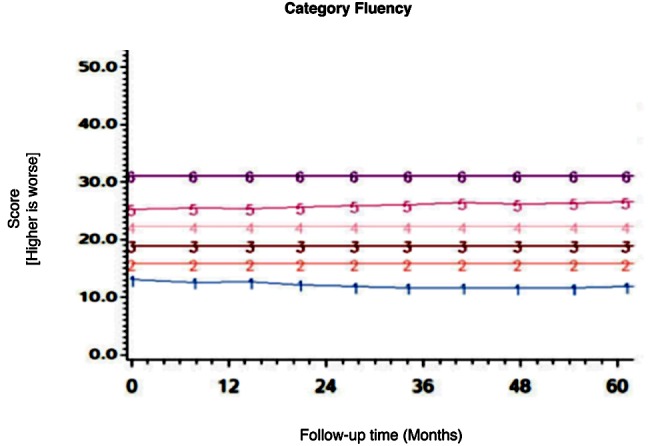
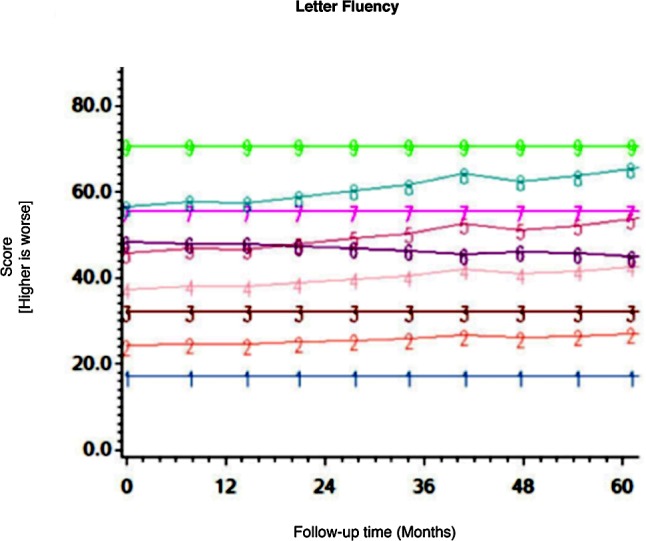
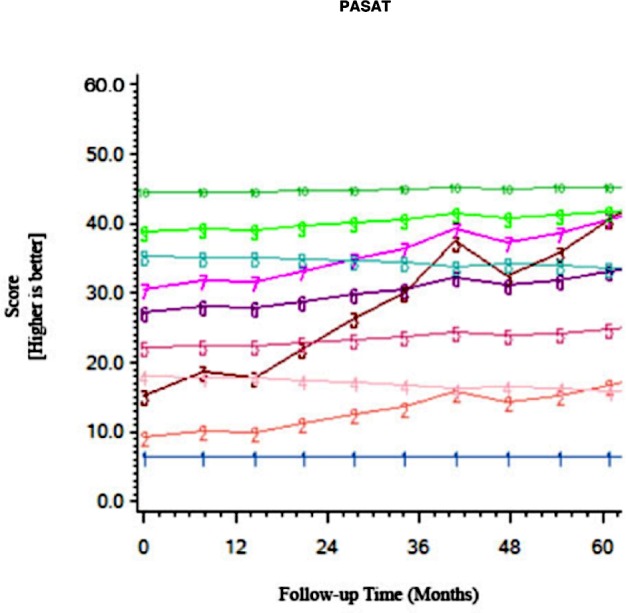
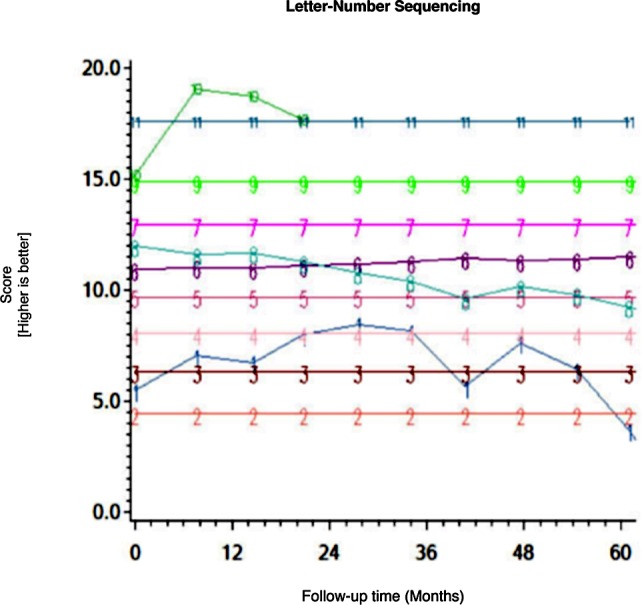
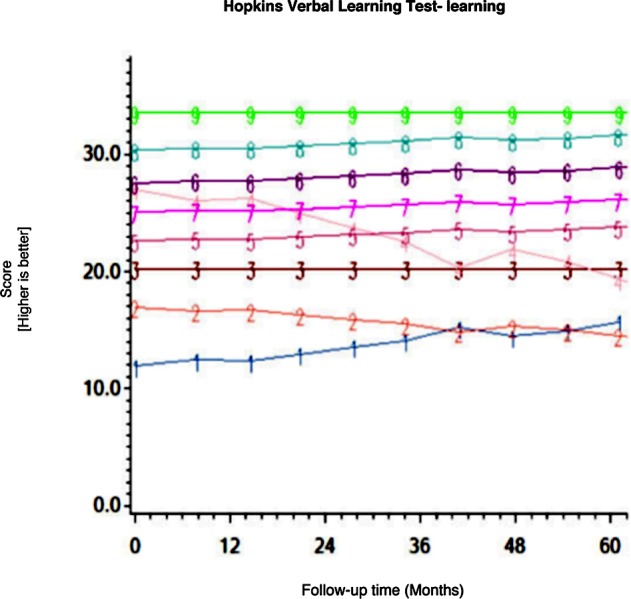
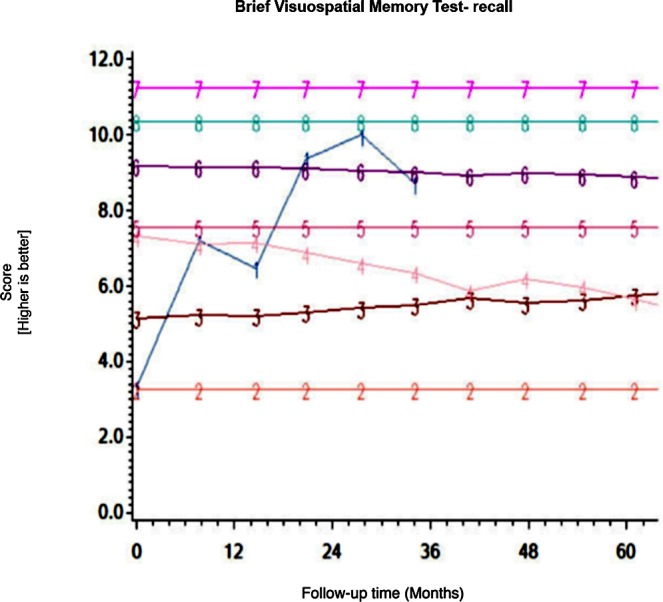
The study population consisted of 701 CHARTER participants who underwent neuropsychological (NP) testing on at least 2 occasions. Raw test scores on 15 NP measures were modeled using GBTA. Each trajectory was categorized as stable, improved or declined, according to two different criteria for change (whether the magnitude of the estimated change at 36 months differed ≥ 0.5 standard deviations from baseline value or changed by > the standard error of measurement estimated at times 1 and 2). Individuals who declined on one or more NP measures were categorized as decliners.
Overall, 111 individuals (15.8%) declined on at least one NP test over 36 months, with the vast majority showing decline on a single NP test (93/111-83.8%). The posterior probability of group assignment was high in most participants (71%) after only 2 sessions, and in the overwhelming majority of those with 3+ sessions. Heterogeneity of trajectories was the norm rather than the exception. Individuals who declined had, on average, worse baseline NP performance on every test, were older, had a longer duration of HIV infection and more follow-up sessions.
The present study identified heterogeneous trajectories over 3 years across 15 NP raw test scores using GBTA. Cognitive decline was observed in only a small subset of this study cohort. Decliners had demographics and HIV characteristics that have been previously associated with cognitive decline, suggesting clinical validity for the method.
尽管联合抗逆转录病毒疗法(cART)已广泛应用,但与HIV相关的神经认知障碍仍然很常见,在纵向神经艾滋病研究中,对神经认知变化轨迹进行调查的研究相对较少。
使用基于群体的轨迹分析(GBTA)对CHARTER队列纵向研究中的参与者进行随访,以估计随访前3年神经认知变化的程度和模式。
研究人群包括701名CHARTER参与者,他们至少接受了2次神经心理学(NP)测试。使用GBTA对15项NP测量的原始测试分数进行建模。根据两种不同的变化标准(36个月时估计变化的幅度与基线值相差是否≥0.5标准差或变化是否大于在第1次和第2次测量时估计的测量标准误差),将每个轨迹分类为稳定、改善或下降。在一项或多项NP测量中出现下降的个体被归类为下降者。
总体而言,111名个体(15.8%)在36个月内至少有一项NP测试出现下降,绝大多数仅在一项NP测试中出现下降(93/111 - 83.8%)。在仅进行2次测试后,大多数参与者(71%)以及绝大多数进行了3次及以上测试的参与者,其分组分配的后验概率都很高。轨迹的异质性是常态而非例外。下降者平均在每项测试中的基线NP表现更差,年龄更大,HIV感染持续时间更长,随访次数更多。
本研究使用GBTA在3年时间内对15项NP原始测试分数确定了异质轨迹。在该研究队列中仅观察到一小部分人出现认知下降。下降者具有先前与认知下降相关的人口统计学和HIV特征,表明该方法具有临床有效性。