Chen Haitao, Liu Xu, Brendler Charles B, Ankerst Donna P, Leach Robin J, Goodman Phyllis J, Lucia M Scott, Tangen Catherine M, Wang Li, Hsu Fang-Chi, Sun Jielin, Kader A Karim, Isaacs William B, Helfand Brian T, Zheng S Lilly, Thompson Ian M, Platz Elizabeth A, Xu Jianfeng
State Key Laboratory of Genetic Engineering, School of Life Science, Fudan University, Shanghai, China.
Center for Cancer Genomics, Wake Forest School of Medicine, Winston-Salem, North Carolina.
Prostate. 2016 Sep;76(12):1120-9. doi: 10.1002/pros.23200. Epub 2016 May 16.
While family history (FH) has been widely used to provide risk information, it captures only a small proportion of subjects with higher genetic susceptibility. Our objective is to assess whether a genetic risk score (GRS) calculated from prostate cancer (PCa) risk-associated single nucleotide polymorphisms (SNPs) can supplement FH for more effective risk stratification for PCa screening decision-making.
A GRS was calculated based on 29 PCa risk-associated SNPs for 4,528 men of European descent in the placebo arm of the Prostate Cancer Prevention Trial (PCPT). At study entry, participants were free of PCa diagnosis. Performance of FH and GRS were measured by observed detection rate of PCa and high-grade PCa (Gleason score ≥7) during the 7-year study.
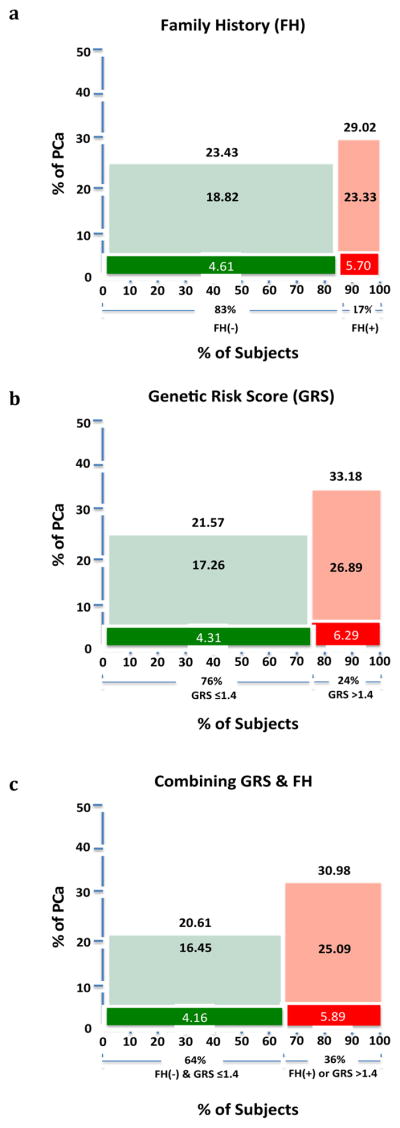
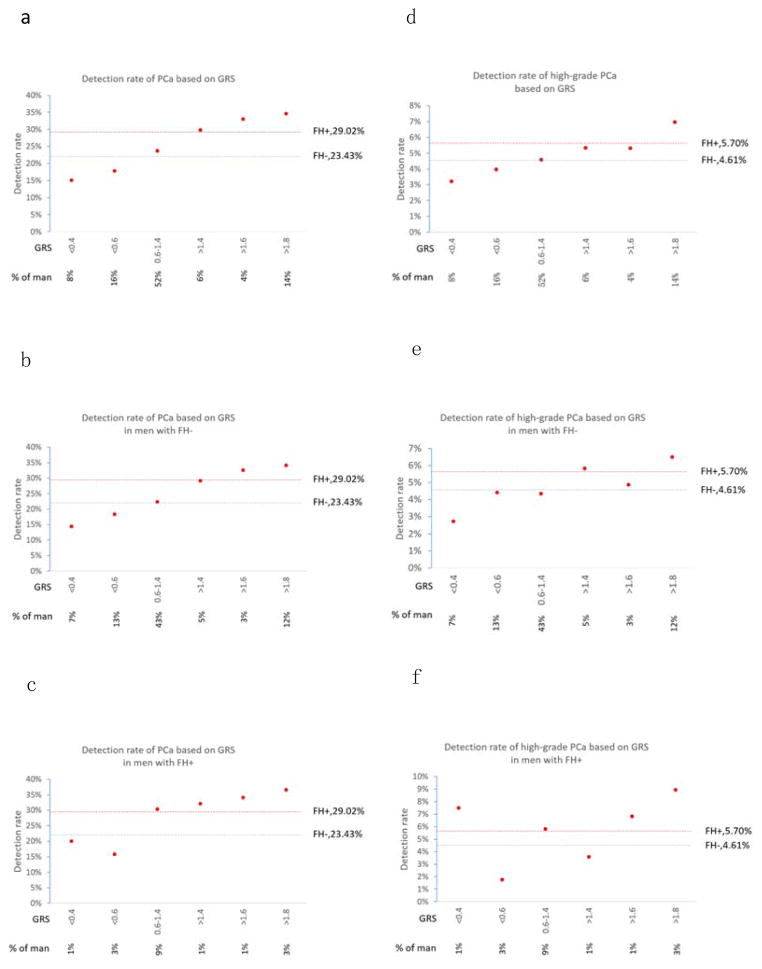
GRS was a significant predictor of PCa in men with or without a positive FH (P = 1.18 × 10(-4) and P = 4.50 × 10(-16) , respectively). Using FH alone, as expected, the 17% of men who were FH+ had a PCa detection rate that was significantly higher (29.02%) than FH- men (23.43%, P = 0.001). When both FH+ or GRS >1.4 are considered, more than twice as many men (36%) can be classified as higher risk, as evidenced by a significantly higher PCa detection rate (30.98%) than in the remaining men (20.61%, P = 5.30 × 10(-15) ). If targeting only FH+ men, four out of five PCa cases would go undetected, as would a similarly large fraction (∼80%) of high-grade PCa cases. In comparison, if targeting FH+ or GRS >1.4 men, almost half of all PCa cases would be detected, including 45% of high-grade PCa cases.
A prostate cancer GRS can supplement family history to better identify higher risk men for targeted intervention. Prostate 76:1120-1129, 2016. © 2016 Wiley Periodicals, Inc.
虽然家族史(FH)已被广泛用于提供风险信息,但它仅涵盖了一小部分遗传易感性较高的个体。我们的目标是评估由前列腺癌(PCa)风险相关单核苷酸多态性(SNP)计算得出的遗传风险评分(GRS)是否可以补充家族史,以便在前列腺癌筛查决策中进行更有效的风险分层。
基于前列腺癌预防试验(PCPT)安慰剂组中4528名欧洲裔男性的29个PCa风险相关SNP计算GRS。在研究开始时,参与者未被诊断出患有PCa。通过在7年研究期间观察到的PCa和高级别PCa(Gleason评分≥7)的检出率来衡量家族史和GRS的表现。
GRS是有或没有阳性家族史男性中PCa的显著预测指标(分别为P = 1.18×10^(-4)和P = 4.50×10^(-16))。正如预期的那样,仅使用家族史时,17%的家族史阳性男性的PCa检出率(29.02%)显著高于家族史阴性男性(23.43%,P = 0.001)。当同时考虑家族史阳性或GRS>1.4时,两倍多的男性(36%)可被归类为高风险,这表现为PCa检出率(30.98%)显著高于其余男性(20.61%,P = 5.30×10^(-15))。如果仅针对家族史阳性男性,五分之四的PCa病例将未被检测到,高级别PCa病例的未被检测到比例也同样高(约80%)。相比之下,如果针对家族史阳性或GRS>1.4的男性,几乎一半的PCa病例将被检测到,包括45%的高级别PCa病例。
前列腺癌GRS可以补充家族史,以更好地识别高风险男性进行有针对性的干预。《前列腺》76:1120 - 1129,2016年。©2016威利期刊公司。