Wong Davie, Wong Titus, Romney Marc, Leung Victor
PGY-V Infectious Diseases Residency Training Program, University of British Columbia, Vancouver General Hospital, D 452 Heather Pavilion, 2733 Heather Street, Vancouver, BC, V5Z 1 M9, Canada.
Department of Pathology and Laboratory Medicine, University of British Columbia, Vancouver, BC, Canada.
BMC Infect Dis. 2016 May 23;16:224. doi: 10.1186/s12879-016-1564-5.
Prior studies suggested that vancomycin may be inferior to β-lactams for the empiric treatment of methicillin-susceptible S. aureus (MSSA) bacteremia. We assessed whether empiric therapy with β-lactams compared to vancomycin was associated with differences in clinical outcomes in patients with MSSA bacteremia.
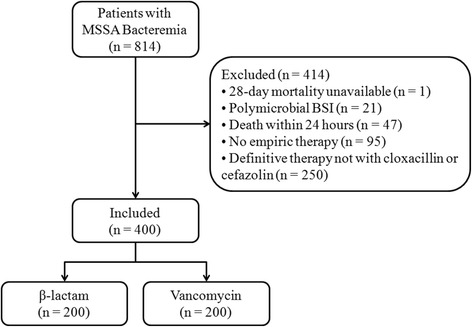
We conducted a retrospective cohort study of adult inpatients with their first episode of MSSA bacteremia at two tertiary care hospitals in Vancouver, Canada, between 2007 and 2014. Exposure was either empiric β-lactam or vancomycin therapy. All patients received definitive treatment with cloxacillin or cefazolin. The primary outcome was 28-day mortality. Secondary outcomes were 90-day mortality, recurrent infection at 6 months, duration of bacteremia and hospital length-of-stay. Outcomes were adjusted using multivariable logistic regression.
Of 814 patients identified, 400 met inclusion criteria (β-lactam = 200, vancomycin = 200). Overall 28-day mortality was 8.5 % (n=34). There were more cases of infective endocarditis in the β-lactam than in the vancomycin group [45 (22.5 %) vs 23 (11.5 %), p < 0.01]. Adjusted mortality at 28 days was similar between the two groups (OR: 1.14; 95 % CI: 0.49-2.64). No differences in secondary outcomes were observed. Transition to cloxacillin or cefazolin occurred within a median of 67.8 h in the vancomycin group.
Empiric therapy with β-lactams was not associated with differences in all-cause mortality, recurrent infection, microbiological cure or hospital length-of-stay compared to vancomycin. Vancomycin monotherapy may be appropriate for the empiric treatment of MSSA bacteremia if definitive therapy with cloxacillin or cefazolin can be initiated within 3 days.
先前的研究表明,在对甲氧西林敏感的金黄色葡萄球菌(MSSA)菌血症进行经验性治疗时,万古霉素可能不如β-内酰胺类药物。我们评估了与万古霉素相比,β-内酰胺类药物的经验性治疗是否与MSSA菌血症患者的临床结局差异相关。
我们对2007年至2014年期间在加拿大温哥华的两家三级护理医院首次发生MSSA菌血症的成年住院患者进行了一项回顾性队列研究。暴露因素为经验性β-内酰胺类药物或万古霉素治疗。所有患者均接受了氯唑西林或头孢唑林的确定性治疗。主要结局为28天死亡率。次要结局为90天死亡率、6个月时的复发性感染、菌血症持续时间和住院时间。结局采用多变量逻辑回归进行调整。
在814名确定的患者中,400名符合纳入标准(β-内酰胺类药物组=200名,万古霉素组=200名)。总体28天死亡率为8.5%(n = 34)。β-内酰胺类药物组的感染性心内膜炎病例比万古霉素组更多[45例(22.5%)对23例(11.5%),p < 0.01]。两组间28天调整后死亡率相似(OR:1.14;95%CI:0.49 - 2.64)。未观察到次要结局的差异。万古霉素组中位67.8小时内转为氯唑西林或头孢唑林治疗。
与万古霉素相比,β-内酰胺类药物的经验性治疗在全因死亡率、复发性感染、微生物学治愈或住院时间方面无差异。如果能在3天内开始用氯唑西林或头孢唑林进行确定性治疗,万古霉素单药治疗可能适用于MSSA菌血症的经验性治疗。