Sayal Parag P, Zafar Arif, Carroll Thomas A
Department of Neurosurgery, The National Hospital for Neurology and Neurosurgery, London, UK.
Department of Neurosurgery, Royal Hallamshire Hospital, Sheffield, UK.
J Craniovertebr Junction Spine. 2016 Apr-Jun;7(2):101-4. doi: 10.4103/0974-8237.181862.
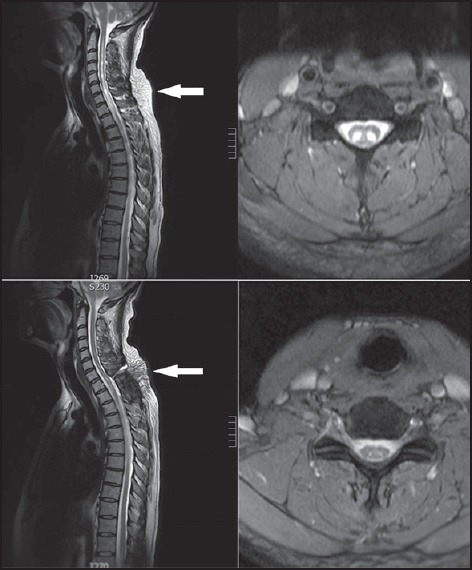
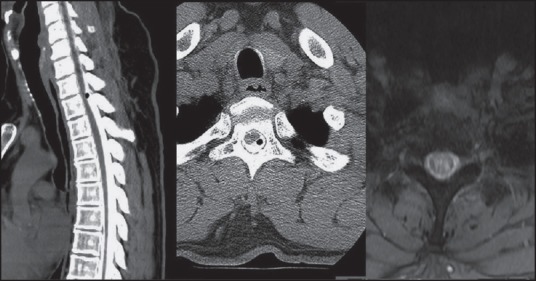
In a certain group of patients with syringomyelia, even with the advent of sophisticated magnetic resonance imaging (MRI), no associated abnormality or cerebrospinal fluid (CSF) block is easily identified. This type of syringomyelia is often termed idiopathic. Current literature has less than 10 reports of arachnoid webs to be the causative factor. We present our experience in the management of two cases of syringomyelia secondary to arachnoid webs. Both our patients presented with progressive neurological deterioration with MRI scans demonstrating cervical/thoracic syrinx without Chiari malformation or low-lying cord. There was no history of previous meningitis or trauma. Both patients underwent myelography that demonstrated dorsal flow block implying CSF obstruction. Cord displacement/change in caliber was also noted and this was not evident on MRI scans. Both patients underwent thoracic laminectomy. After opening the dura, thickened/abnormal arachnoid tissue was found that was resected thus widely communicating the dorsal subarachnoid space. Postoperatively at 6 months, both patients had significant symptomatic improvement with follow-up MRI scans demonstrating significant resolution of the syrinx. In patients with presumed idiopathic syringomyelia, imaging studies should be closely inspected for the presence of a transverse arachnoid web. We believe that all patients with idiopathic symptomatic syringomyelia should have MRI CSF flow studies and/or computed tomography (CT) myelography to identify such arachnoid abnormalities that are often underdiagnosed. Subsequent surgery should be directed at the establishment of normal CSF flow by laminectomy and excision of the offending arachnoid tissue.
在某组脊髓空洞症患者中,即使先进的磁共振成像(MRI)出现了,也很难轻易识别出相关异常或脑脊液(CSF)梗阻。这种类型的脊髓空洞症通常被称为特发性。目前文献中关于蛛网膜粘连为致病因素的报道不足10例。我们介绍我们治疗两例由蛛网膜粘连引起的脊髓空洞症的经验。我们的两名患者均表现为进行性神经功能恶化,MRI扫描显示颈段/胸段脊髓空洞,无Chiari畸形或脊髓低位。既往无脑膜炎或外伤史。两名患者均接受了脊髓造影,显示背侧血流受阻,提示脑脊液梗阻。还注意到脊髓移位/管径变化,而这在MRI扫描中并不明显。两名患者均接受了胸椎椎板切除术。打开硬脑膜后,发现增厚/异常的蛛网膜组织并予以切除,从而使背侧蛛网膜下腔广泛相通。术后6个月,两名患者症状均有显著改善,随访MRI扫描显示脊髓空洞明显消退。对于疑似特发性脊髓空洞症患者,应仔细检查影像学研究以确定是否存在横向蛛网膜粘连。我们认为,所有特发性症状性脊髓空洞症患者均应进行MRI脑脊液流动研究和/或计算机断层扫描(CT)脊髓造影,以识别这种常被漏诊的蛛网膜异常。后续手术应通过椎板切除术和切除病变蛛网膜组织来建立正常的脑脊液流动。