Hong Jae-Seok, Yi Sang-Wook, Yi Jee-Jeon, Hong Seri, Ohrr Heechoul
From the Department of Healthcare Management, Cheongju University College of Health Sciences, Cheongju (J-SH); Department of Preventive Medicine and Public Health, Catholic Kwandong University College of Medicine, Gangneung (S-WY); Institute for Clinical and Translational Research (S-WY), Institute for Occupational and Environmental Health, Catholic Kwandong University, Gangneung (J-JY); Department of Preventive Medicine, Graduate School of Public Health, Yonsei University, Seoul (SH); Institute for Health Promotion, Graduate School of Public Health, Yonsei University, Seoul (HO); and Department of Preventive Medicine, Yonsei University College of Medicine (HO), Seoul, Republic of Korea.
Medicine (Baltimore). 2016 May;95(21):e3684. doi: 10.1097/MD.0000000000003684.
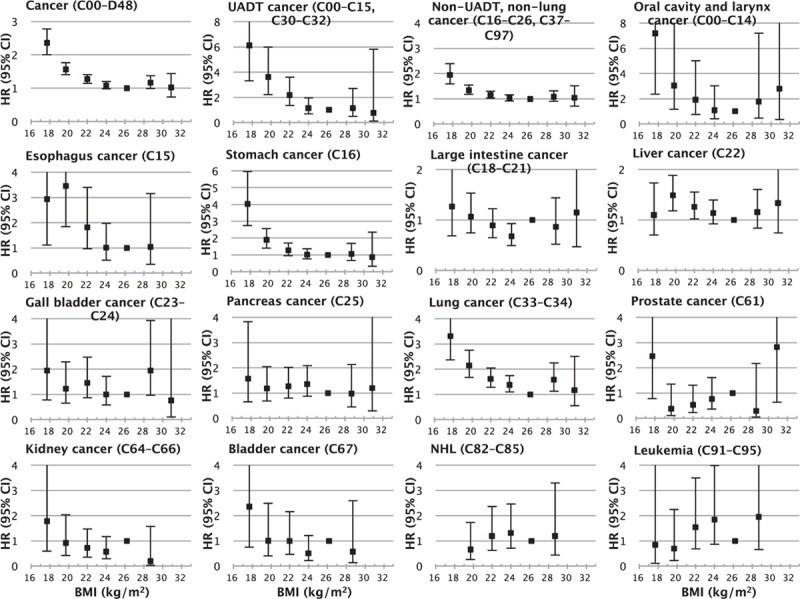
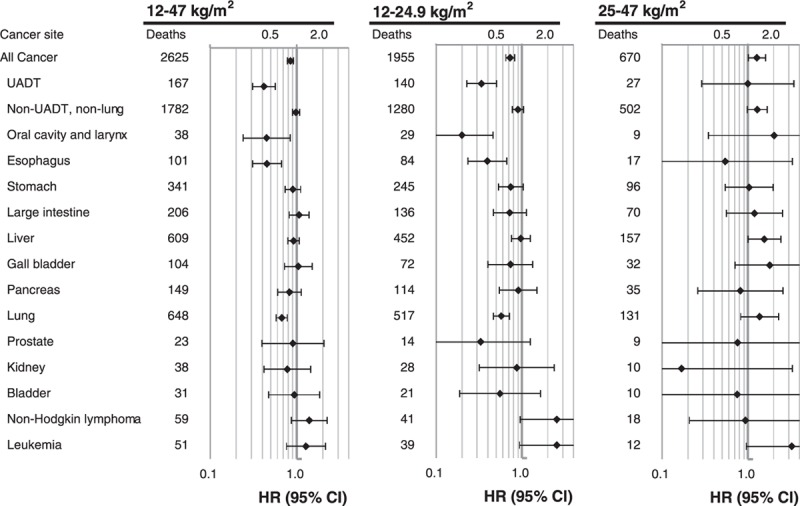
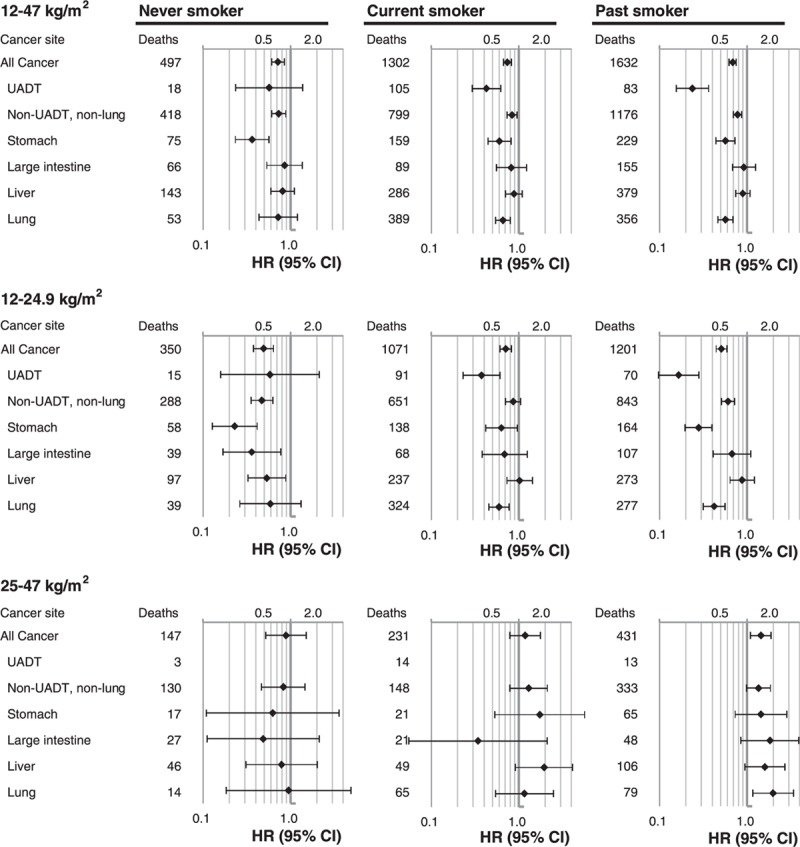
The association of body mass index (BMI; kg/m) with overall and site-specific cancer mortality in Asians is not well understood. A total of 113,478 men from the Korean Veterans Health Study who returned a postal survey in 2004 were followed up until 2010. The adjusted hazard ratios (HRs) of cancer mortality were calculated using a Cox model. During 6.4 years of follow-up, 3478 men died from cancer. A reverse J-curve association with a nadir at 25.0 to 27.4 kg/m was observed. Below 25 kg/m, the HRs of death for each 5 kg/m decrease in BMI were 1.72 (95% confidence interval = 1.57-1.90) for overall cancer; 3.63 (2.57-5.12) for upper aerodigestive tract (UADT) cancers, including oral cavity and larynx [HR = 4.21 (2.18-8.12)] and esophagus [HR = 2.96 (1.82-4.81)] cancers; 1.52 (1.35-1.71) for non-UADT and non-lung cancers, including stomach [HR = 2.72 (2.13-3.48)] and large intestine [HR = 1.68 (1.20-2.36)] cancers; and 1.93 (1.59-2.34) for lung cancer. In the range of 25 to 47 kg/m, the HRs for each 5 kg/m increase in BMI were 1.27 (1.03-1.56) for overall cancer mortality and 1.57 (1.02-2.43) for lung cancer mortality. In individuals <25 kg/m, inverse associations with mortality from overall cancer and non-UADT and non-lung cancer were stronger in never-smokers than in current smokers. Both low and high BMI were strong predictors of mortality from overall and several site-specific cancers in Korean men. Further research is needed to evaluate whether interventions involving weight change (loss or gain) reduce the risk of cancer or improve the survival.
体重指数(BMI;千克/米²)与亚洲人总体及特定部位癌症死亡率之间的关联尚未完全明确。对韩国退伍军人健康研究中2004年回复邮寄调查问卷的113478名男性进行随访,直至2010年。使用Cox模型计算癌症死亡率的校正风险比(HR)。在6.4年的随访期间,3478名男性死于癌症。观察到呈反向J曲线关联,最低点在25.0至27.4千克/米²之间。BMI低于25千克/米²时,BMI每降低5千克/米²,总体癌症死亡的HR为1.72(95%置信区间=1.57 - 1.90);上呼吸消化道(UADT)癌症(包括口腔和喉癌[HR = 4.21(2.18 - 8.12)]和食管癌[HR = 2.96(1.82 - 4.81)])死亡的HR为3.63(2.57 - 5.12);非UADT和非肺癌(包括胃癌[HR = 2.72(2.13 - 3.48)]和大肠癌[HR = 1.68(1.20 - 2.36)])死亡的HR为1.52(1.35 - 1.71);肺癌死亡的HR为1.93(1.59 - 2.34)。在25至47千克/米²范围内,BMI每增加5千克/米²,总体癌症死亡率的HR为1.27(1.03 - 1.56),肺癌死亡率的HR为1.57(1.02 - 2.43)。在BMI<25千克/米²的个体中,从不吸烟者总体癌症及非UADT和非肺癌死亡率的反向关联比当前吸烟者更强。低BMI和高BMI都是韩国男性总体及几种特定部位癌症死亡率的强预测因素。需要进一步研究以评估涉及体重变化(减轻或增加)的干预措施是否能降低癌症风险或改善生存率。