Sepulveda Esteban, Franco José G, Trzepacz Paula T, Gaviria Ana M, Meagher David J, Palma José, Viñuelas Eva, Grau Imma, Vilella Elisabet, de Pablo Joan
Hospital Psiquiatric Universitari Institut Pere Mata, IISPV, Universitat Rovira i Virgili, Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Reus, Tarragona, Spain.
Grupo de Investigación en Psiquiatría de Enlace, Escuela de Ciencias de la Salud, Facultad de Medicina, Universidad Pontificia Bolivariana, Medellín, Colombia.
BMC Psychiatry. 2016 May 26;16:167. doi: 10.1186/s12888-016-0878-6.
Information on validity and reliability of delirium criteria is necessary for clinicians, researchers, and further developments of DSM or ICD. We compare four DSM and ICD delirium diagnostic criteria versions, which were developed by consensus of experts, with a phenomenology-based natural diagnosis delineated using cluster analysis of delirium features in a sample with a high prevalence of dementia. We also measured inter-rater reliability of each system when applied by two evaluators from distinct disciplines.
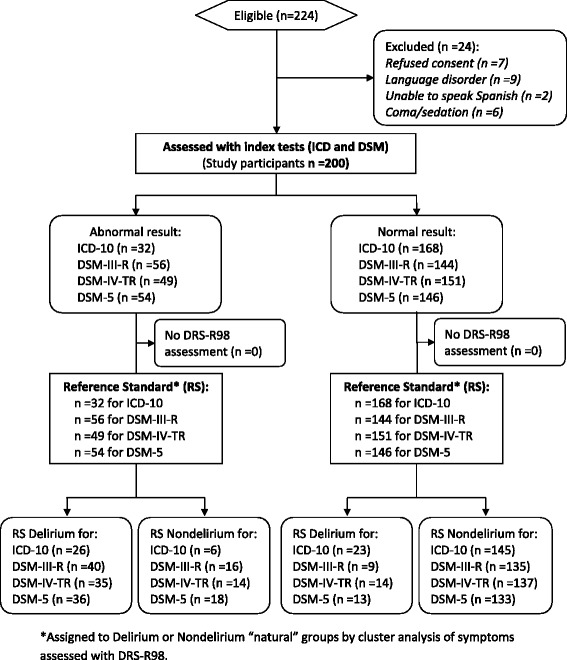
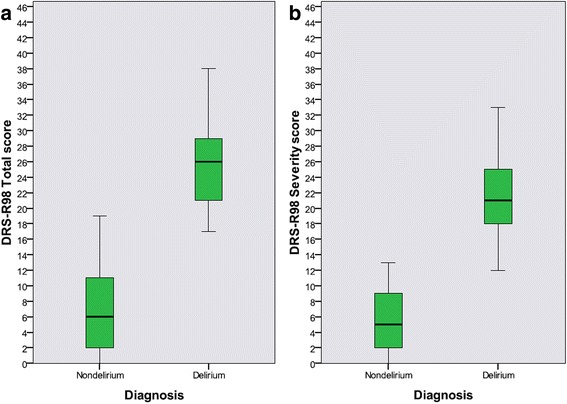
Cross-sectional analysis of 200 consecutive patients admitted to a skilled nursing facility, independently assessed within 24-48 h after admission with the Delirium Rating Scale-Revised-98 (DRS-R98) and for DSM-III-R, DSM-IV, DSM-5, and ICD-10 criteria for delirium. Cluster analysis (CA) delineated natural delirium and nondelirium reference groups using DRS-R98 items and then diagnostic systems' performance were evaluated against the CA-defined groups using logistic regression and crosstabs for discriminant analysis (sensitivity, specificity, percentage of subjects correctly classified by each diagnostic system and their individual criteria, and performance for each system when excluding each individual criterion are reported). Kappa Index (K) was used to report inter-rater reliability for delirium diagnostic systems and their individual criteria.
117 (58.5 %) patients had preexisting dementia according to the Informant Questionnaire on Cognitive Decline in the Elderly. CA delineated 49 delirium subjects and 151 nondelirium. Against these CA groups, delirium diagnosis accuracy was highest using DSM-III-R (87.5 %) followed closely by DSM-IV (86.0 %), ICD-10 (85.5 %) and DSM-5 (84.5 %). ICD-10 had the highest specificity (96.0 %) but lowest sensitivity (53.1 %). DSM-III-R had the best sensitivity (81.6 %) and the best sensitivity-specificity balance. DSM-5 had the highest inter-rater reliability (K =0.73) while DSM-III-R criteria were the least reliable.
Using our CA-defined, phenomenologically-based delirium designations as the reference standard, we found performance discordance among four diagnostic systems when tested in subjects where comorbid dementia was prevalent. The most complex diagnostic systems have higher accuracy and the newer DSM-5 have higher reliability. Our novel phenomenological approach to designing a delirium reference standard may be preferred to guide revisions of diagnostic systems in the future.
谵妄诊断标准的有效性和可靠性信息对于临床医生、研究人员以及《精神疾病诊断与统计手册》(DSM)或《国际疾病分类》(ICD)的进一步发展至关重要。我们将四个由专家共识制定的DSM和ICD谵妄诊断标准版本,与通过对痴呆高患病率样本中的谵妄特征进行聚类分析得出的基于现象学的自然诊断进行比较。我们还测量了两个来自不同学科的评估者应用每个系统时的评分者间信度。
对连续入住一家专业护理机构的200例患者进行横断面分析,在入院后24 - 48小时内使用修订版谵妄评定量表(DRS - R98)以及DSM - III - R、DSM - IV、DSM - 5和ICD - 10的谵妄标准进行独立评估。聚类分析(CA)使用DRS - R98项目划分出自然谵妄和非谵妄参考组,然后使用逻辑回归和交叉表进行判别分析,针对CA定义的组评估诊断系统的性能(报告每个诊断系统及其各自标准的敏感性、特异性、正确分类的受试者百分比,以及排除每个单独标准时每个系统的性能)。kappa指数(K)用于报告谵妄诊断系统及其各自标准的评分者间信度。
根据老年人认知下降 informant问卷,117例(58.5%)患者患有既往痴呆。CA划分出49例谵妄患者和151例非谵妄患者。与这些CA组相比,使用DSM - III - R进行谵妄诊断的准确性最高(87.5%),其次是DSM - IV(86.)、ICD - 10(85.5%)和DSM - 5(84.5%)。ICD - 10具有最高的特异性(96.0%)但最低的敏感性(53.1%)。DSM - III - R具有最佳的敏感性(81.6%)和最佳的敏感性 - 特异性平衡。DSM - 5具有最高的评分者间信度(K = 0.73),而DSM - III - R标准的信度最低。
以我们基于现象学通过CA定义的谵妄分类作为参考标准,我们发现在合并痴呆症患病率较高的受试者中进行测试时,四个诊断系统之间存在性能差异。最复杂的诊断系统具有更高的准确性,而较新的DSM - 5具有更高的信度。我们设计谵妄参考标准的新颖现象学方法可能更适合指导未来诊断系统修订。