Florman S, Becker T, Bresnahan B, Chevaile-Ramos A, Carvalho D, Grannas G, Muehlbacher F, O'Connell P J, Meier-Kriesche H U, Larsen C P
Recanti/Miller Transplant Institute, Mount Sinai Medical Center, New York, NY.
Clinic for General Surgery, Visceral, Thoracic, Transplantation and Pediatric Surgery, University Hospital Schleswig-Holstein, Kiel, Germany.
Am J Transplant. 2017 Jan;17(1):180-190. doi: 10.1111/ajt.13886. Epub 2016 Jul 12.
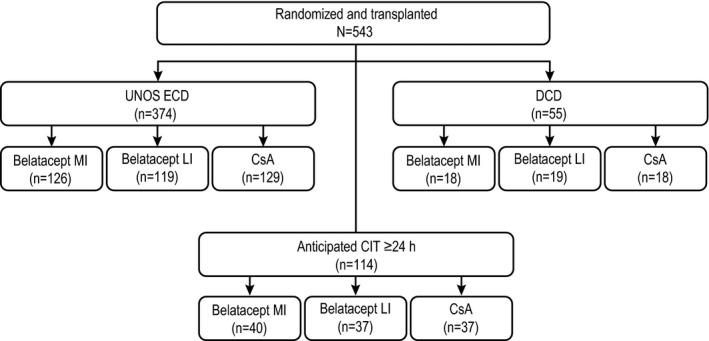
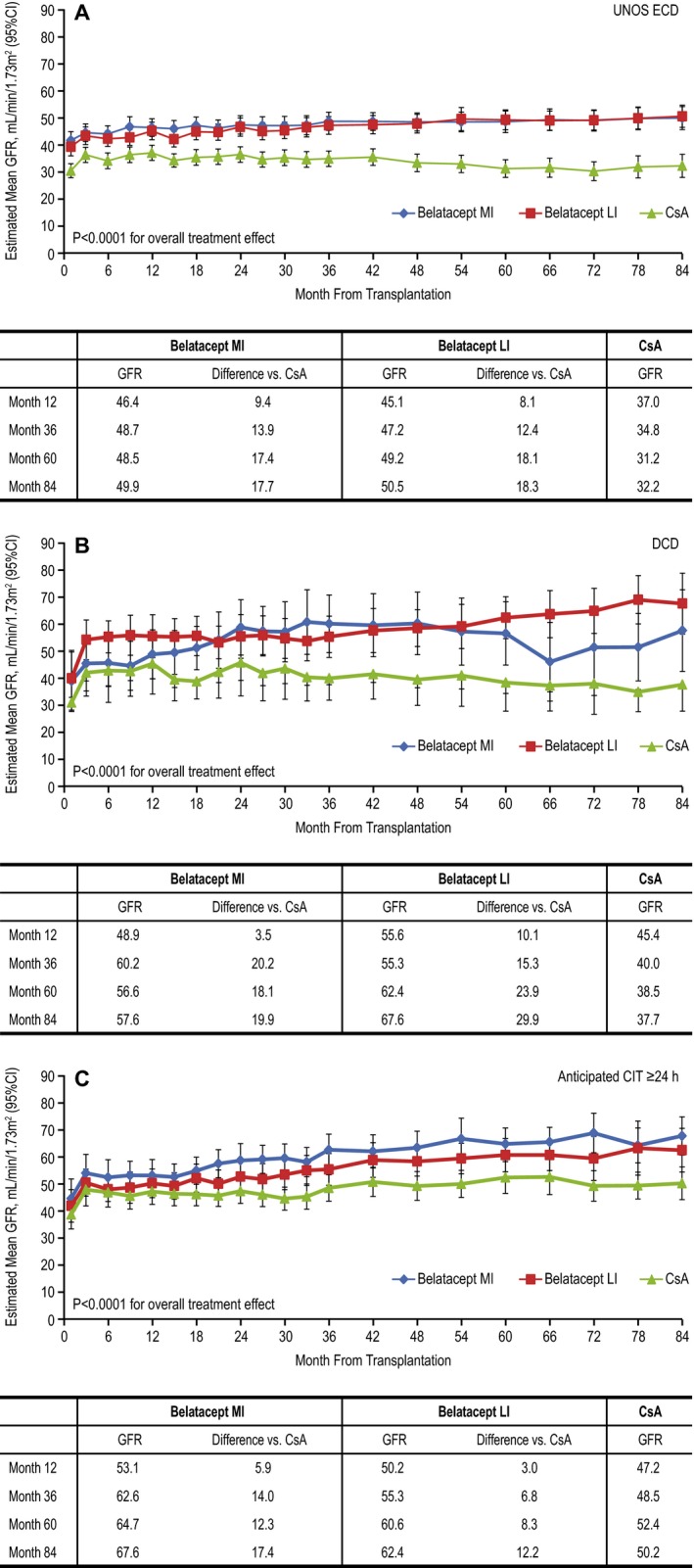
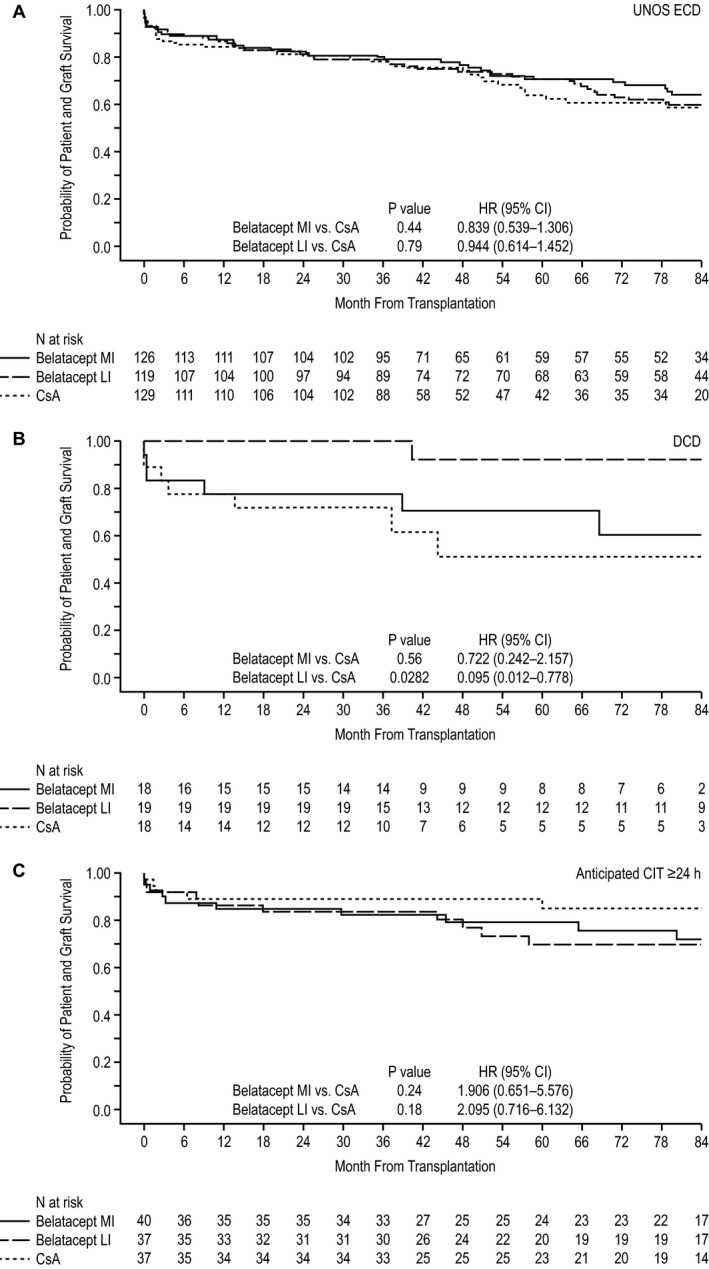
The phase III Belatacept Evaluation of Nephroprotection and Efficacy as First-Line Immunosuppression Trial-Extended Criteria Donors Trial (BENEFIT-EXT) study compared more or less intensive belatacept-based immunosuppression with cyclosporine (CsA)-based immunosuppression in recipients of extended criteria donor kidneys. In this post hoc analysis, patient outcomes were assessed according to donor kidney subtype. In total, 68.9% of patients received an expanded criteria donor kidney (United Network for Organ Sharing definition), 10.1% received a donation after cardiac death kidney, and 21.0% received a kidney with an anticipated cold ischemic time ≥24 h. Over 7 years, time to death or graft loss was similar between belatacept- and CsA-based immunosuppression, regardless of donor kidney subtype. In all three donor kidney cohorts, estimated mean GFR increased over months 1-84 for belatacept-based treatment but declined for CsA-based treatment. The estimated differences in GFR significantly favored each belatacept-based regimen versus the CsA-based regimen in the three subgroups (p < 0.0001 for overall treatment effect). No differences in the safety profile of belatacept were observed by donor kidney subtype.
III期贝拉西普作为一线免疫抑制的肾保护和疗效评估试验——扩大标准供体试验(BENEFIT-EXT)研究,比较了接受扩大标准供体肾脏的受者中,基于贝拉西普的免疫抑制与基于环孢素(CsA)的免疫抑制,二者强度或多或少有所不同。在这项事后分析中,根据供体肾脏亚型评估患者预后。总体而言,68.9%的患者接受了扩大标准供体肾脏(器官共享联合网络定义),10.1%的患者接受了心脏死亡后捐赠的肾脏,21.0%的患者接受了预期冷缺血时间≥24小时的肾脏。在7年多的时间里,无论供体肾脏亚型如何,基于贝拉西普的免疫抑制和基于CsA的免疫抑制在死亡或移植物丢失时间方面相似。在所有三个供体肾脏队列中,基于贝拉西普的治疗在第1至84个月时估计平均肾小球滤过率(GFR)升高,而基于CsA的治疗则下降。在三个亚组中,基于贝拉西普的每种方案的GFR估计差异显著优于基于CsA的方案(总体治疗效果p<0.0001)。未观察到供体肾脏亚型对贝拉西普安全性的影响存在差异。