Brown Steven R, Tiernan James P, Watson Angus J M, Biggs Katie, Shephard Neil, Wailoo Allan J, Bradburn Mike, Alshreef Abualbishr, Hind Daniel
Sheffield Teaching Hospitals, Sheffield, UK.
St James's University Hospital, Leeds, UK.
Lancet. 2016 Jul 23;388(10042):356-364. doi: 10.1016/S0140-6736(16)30584-0. Epub 2016 May 25.
Optimum surgical intervention for low-grade haemorrhoids is unknown. Haemorrhoidal artery ligation (HAL) has been proposed as an efficacious, safe therapy while rubber band ligation (RBL) is a commonly used outpatient treatment. We compared recurrence after HAL versus RBL in patients with grade II-III haemorrhoids.
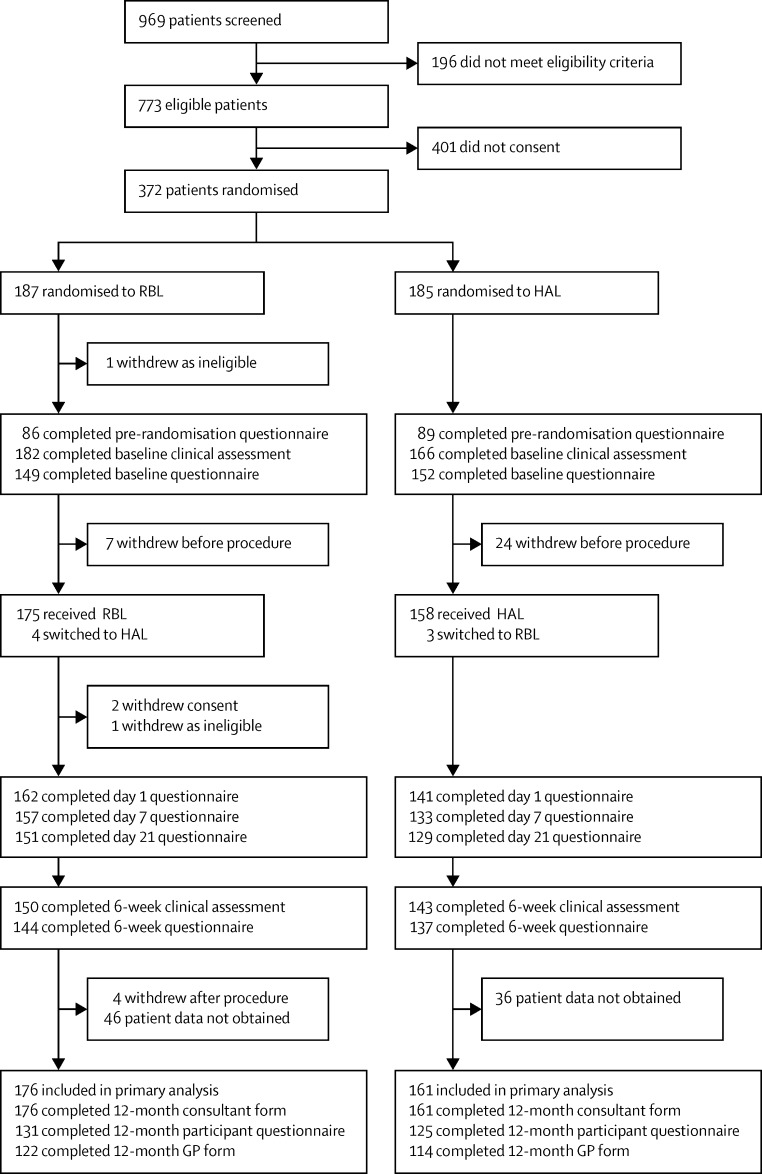
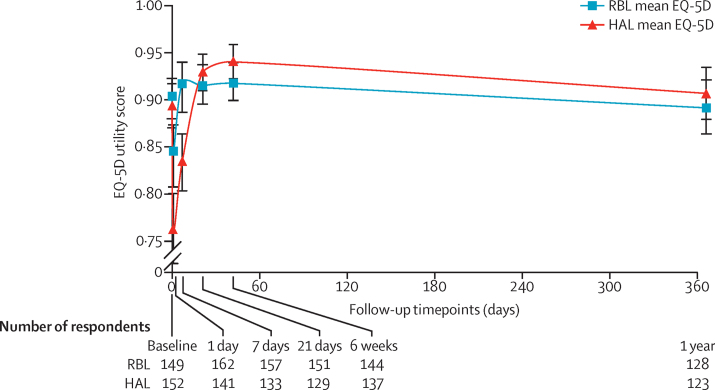
This multicentre, open-label, parallel group, randomised controlled trial included patients from 17 acute UK NHS trusts. We screened patients aged 18 years or older presenting with grade II-III haemorrhoids. We excluded patients who had previously received any haemorrhoid surgery, more than one injection treatment for haemorrhoids, or more than one RBL procedure within 3 years before recruitment. Eligible patients were randomly assigned (in a 1:1 ratio) to either RBL or HAL with Doppler. Randomisation was computer-generated and stratified by centre with blocks of random sizes. Allocation concealment was achieved using a web-based system. The study was open-label with no masking of participants, clinicians, or research staff. The primary outcome was recurrence at 1 year, derived from the patient's self-reported assessment in combination with resource use from their general practitioner and hospital records. Recurrence was analysed in patients who had undergone one of the interventions and been followed up for at least 1 year. This study is registered with the ISRCTN registry, ISRCTN41394716.
From Sept 9, 2012, to May 6, 2014, of 969 patients screened, 185 were randomly assigned to the HAL group and 187 to the RBL group. Of these participants, 337 had primary outcome data (176 in the RBL group and 161 in the HAL group). At 1 year post-procedure, 87 (49%) of 176 patients in the RBL group and 48 (30%) of 161 patients in the HAL group had haemorrhoid recurrence (adjusted odds ratio [aOR] 2·23, 95% CI 1·42-3·51; p=0·0005). The main reason for this difference was the number of extra procedures required to achieve improvement (57 [32%] participants in the RBL group and 23 [14%] participants in the HAL group had a subsequent procedure for haemorrhoids). The mean pain 1 day after procedure was 3·4 (SD 2·8) in the RBL group and 4·6 (2·8) in the HAL group (difference -1·2, 95% CI -1·8 to -0·5; p=0·0002); at day 7 the scores were 1·6 (2·3) in the RBL group and 3·1 (2·4) in the HAL group (difference -1·5, -2·0 to -1·0; p<0·0001). Pain scores did not differ between groups at 21 days and 6 weeks. 15 individuals reported serious adverse events requiring hospital admission. One patient in the RBL group had a pre-existing rectal tumour. Of the remaining 14 serious adverse events, 12 (7%) were among participants treated with HAL and two (1%) were in those treated with RBL. Six patients had pain (one treated with RBL, five treated with HAL), three had bleeding not requiring transfusion (one treated with RBL, two treated with HAL), two in the HAL group had urinary retention, two in the HAL group had vasovagal upset, and one in the HAL group had possible sepsis (treated with antibiotics).
Although recurrence after HAL was lower than a single RBL, HAL was more painful than RBL. The difference in recurrence was due to the need for repeat bandings in the RBL group. Patients (and health commissioners) might prefer such a course of RBL to the more invasive HAL.
NIHR Health Technology Assessment programme.
对于轻度痔疮的最佳手术干预方式尚不清楚。有人提出痔动脉结扎术(HAL)是一种有效、安全的治疗方法,而橡皮圈套扎术(RBL)是常用的门诊治疗手段。我们比较了II-III度痔疮患者接受HAL与RBL治疗后的复发情况。
这项多中心、开放标签、平行组随机对照试验纳入了来自英国17个急性国民保健服务信托机构的患者。我们筛选了年龄在18岁及以上的II-III度痔疮患者。我们排除了在招募前3年内曾接受过任何痔疮手术、接受过不止一次痔疮注射治疗或不止一次RBL手术的患者。符合条件的患者以1:1的比例随机分配至RBL组或使用多普勒的HAL组。随机分组由计算机生成,并按中心分层,随机分组块大小不等。使用基于网络的系统实现分配隐藏。该研究为开放标签,不对参与者、临床医生或研究人员进行盲法。主要结局是1年时的复发情况,通过患者的自我报告评估结合其全科医生和医院记录中的资源使用情况得出。对接受了其中一种干预措施并随访至少1年的患者进行复发情况分析。本研究已在国际标准随机对照试验编号注册库(ISRCTN registry)注册,注册号为ISRCTN41394716。
从2012年9月9日至2014年5月6日,在969名筛查的患者中,185名被随机分配至HAL组,187名被随机分配至RBL组。在这些参与者中,337名有主要结局数据(RBL组176名,HAL组161名)。术后1年,RBL组176名患者中有87名(49%)出现痔疮复发,HAL组161名患者中有48名(30%)出现复发(调整优势比[aOR]为2.23,95%置信区间为1.42 - 3.51;p = 0.0005)。造成这种差异的主要原因是为实现病情改善所需的额外手术次数(RBL组57名[32%]参与者,HAL组23名[14%]参与者随后接受了痔疮相关手术)。术后1天,RBL组的平均疼痛评分为3.4(标准差2.8),HAL组为4.6(2.8)(差异为-1.2,95%置信区间为-1.8至-0.5;p = 0.0002);第7天时,RBL组评分为1.6(2.3),HAL组为3.1(2.4)(差异为-1.5,-2.0至-1.0;p < 0.0001)。21天和6周时两组疼痛评分无差异。15名个体报告了需要住院治疗的严重不良事件。RBL组有1名患者存在直肠肿瘤。在其余14起严重不良事件中,12起(7%)发生在接受HAL治疗组的参与者中,2起(1%)发生在接受RBL治疗组的参与者中。6名患者出现疼痛(1名接受RBL治疗,5名接受HAL治疗),3名出现无需输血的出血情况(1名接受RBL治疗,2名接受HAL治疗),HAL组有2名患者出现尿潴留,HAL组有2名患者出现血管迷走性不适,HAL组有1名患者可能发生了脓毒症(接受了抗生素治疗)。
虽然HAL术后复发率低于单次RBL,但HAL比RBL更疼痛。复发差异是由于RBL组需要重复套扎。患者(以及卫生保健专员)可能更倾向于选择RBL这种治疗方式而非侵入性更强的HAL。
英国国家卫生研究院卫生技术评估项目。