Legrand Matthieu, Le Cam Brigitte, Perbet Sébastien, Roger Claire, Darmon Michael, Guerci Philippe, Ferry Axelle, Maurel Véronique, Soussi Sabri, Constantin Jean-Michel, Gayat Etienne, Lefrant Jean-Yves, Leone Marc
AP-HP, GH St-Louis-Lariboisière, Anesthésie, Réanimation et brûlés, Hôpital St-Louis, Assistance Publique-Hôpitaux de Paris, 1 rue Claude Vellefaux, 75010, Paris, France.
UMR INSERM 942, Institut National de la Santé et de la Recherche Médicale (INSERM), Lariboisière Hospital, Paris, France.
Crit Care. 2016 May 29;20(1):165. doi: 10.1186/s13054-016-1343-0.
Oliguria is one of the leading triggers of fluid loading in patients in the intensive care unit (ICU). The purpose of this study was to assess the predictive value of urine Na(+) (uNa(+)) and other routine urine biomarkers for cardiac fluid responsiveness in oliguric ICU patients.
We conducted a prospective multicenter observational study in five university ICUs. Patients with urine output (UO) <0.5 ml/kg/h for 3 consecutive hours with a mean arterial pressure >65 mmHg received a fluid challenge. Cardiac fluid responsiveness was defined by an increase in stroke volume >15 % after fluid challenge. Urine and plasma biochemistry samples were examined before fluid challenge. We examined renal fluid responsiveness (defined as UO > 0.5 ml/kg/h for 3 consecutive hours) after fluid challenge as a secondary endpoint.
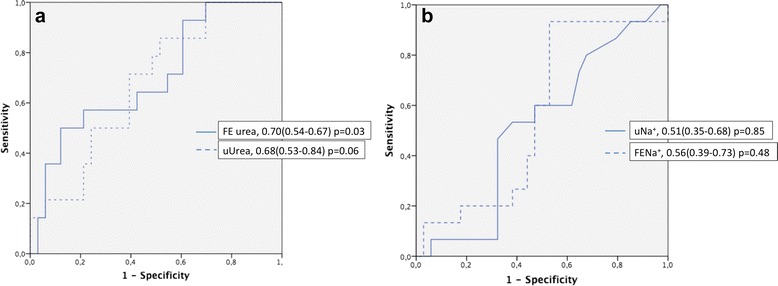
Fifty-four patients (age 51 ± 37 years, Simplified Acute Physiology Score II score 40 ± 20) were included. Most patients (72 %) were not cardiac responders (CRs), and 50 % were renal responders (RRs) to fluid challenge. Patient characteristics were similar between CRs and cardiac nonresponders. uNa(+) (37 ± 38 mmol/L vs 25 ± 75 mmol/L, p = 0.44) and fractional excretion of sodium (FENa(+)) (2.27 ± 2.5 % vs 2.15 ± 5.0 %, p = 0.94) were not statistically different between those who did and those who did not respond to the fluid challenge. Areas under the receiver operating characteristic (AUROC) curves were 0.51 (95 % CI 0.35-0.68) and 0.56 (95 % CI 0.39-0.73) for uNa(+) and FENa(+), respectively. Fractional excretion of urea had an AUROC curve of 0.70 (95 % CI 0.54-0.86, p = 0.03) for CRs. Baseline UO was higher in RRs than in renal nonresponders (1.07 ± 0.78 ml/kg/3 h vs 0.65 ± 0.53 ml/kg/3 h, p = 0.01). The AUROC curve for RRs was 0.65 (95 % CI 0.53-0.78) for uNa(+).
In the present study, most oliguric patients were not CRs and half were not renal responders to fluid challenge. Routine urinary biomarkers were not predictive of fluid responsiveness in oliguric normotensive ICU patients.
少尿是重症监护病房(ICU)患者液体负荷增加的主要诱因之一。本研究旨在评估少尿的ICU患者尿钠(uNa(+))及其他常规尿液生物标志物对心脏液体反应性的预测价值。
我们在五所大学的ICU进行了一项前瞻性多中心观察性研究。平均动脉压>65 mmHg且尿量(UO)连续3小时<0.5 ml/kg/h的患者接受液体冲击试验。心脏液体反应性定义为液体冲击试验后每搏输出量增加>15%。在液体冲击试验前检测尿液和血浆生化样本。我们将液体冲击试验后肾液体反应性(定义为UO连续3小时>0.5 ml/kg/h)作为次要终点进行检测。
纳入54例患者(年龄51±37岁,简化急性生理学评分II为40±20)。大多数患者(72%)对液体冲击试验无心脏反应(CRs),50%对液体冲击试验有肾脏反应(RRs)。CRs与无心脏反应者的患者特征相似。有或无液体反应者之间的uNa(+)(37±38 mmol/L对25±75 mmol/L,p = 0.44)和钠排泄分数(FENa(+))(2.27±2.5%对2.15±5.0%,p = 0.94)无统计学差异。uNa(+)和FENa(+)的受试者工作特征(AUROC)曲线下面积分别为0.51(95%CI 0.35 - 0.68)和0.56(95%CI 0.39 - 0.73)。尿素排泄分数对CRs的AUROC曲线为0.70(95%CI 0.54 - 0.86,p = 0.03)。RRs的基线UO高于无肾脏反应者(1.07±0.78 ml/kg/3 h对0.65±0.53 ml/kg/3 h,p = 0.01)。uNa(+)对RRs的AUROC曲线为0.65(95%CI 0.53 - 0.78)。
在本研究中,大多数少尿患者对液体冲击试验无CRs,半数对液体冲击试验无肾脏反应。常规尿液生物标志物不能预测少尿且血压正常的ICU患者的液体反应性。