Hashemi Hassan, Beiranvand Asghar, Yekta Abbasali, Maleki Azam, Yazdani Negareh, Khabazkhoob Mehdi
Noor Research Center for Ophthalmic Epidemiology, Noor Eye Hospital, Tehran, Iran.
Health and nutrition Research Center, Lorestan University of Medical Sciences, Khoramabad, Iran.
J Curr Ophthalmol. 2016 Mar 29;28(1):21-6. doi: 10.1016/j.joco.2016.01.009. eCollection 2016 Mar.
To determine pachymetric, aberrometric, and topometric indices in patients with definite and subclinical keratoconus and the validity of these indices in the diagnosis of keratoconus.
We evaluated 262 keratoconic and 97 healthy eyes in this study. Pentacam HR examination was performed for all participants, and the data of all pachymetric, aberrometric, and topometric indices was extracted for the study population.
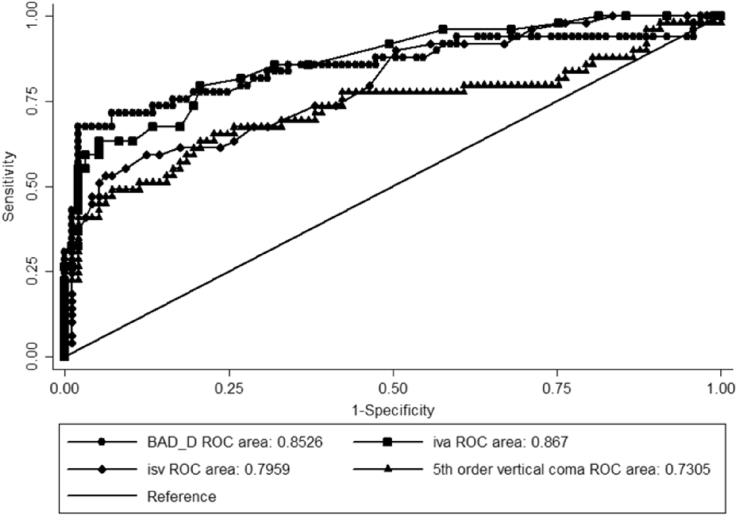
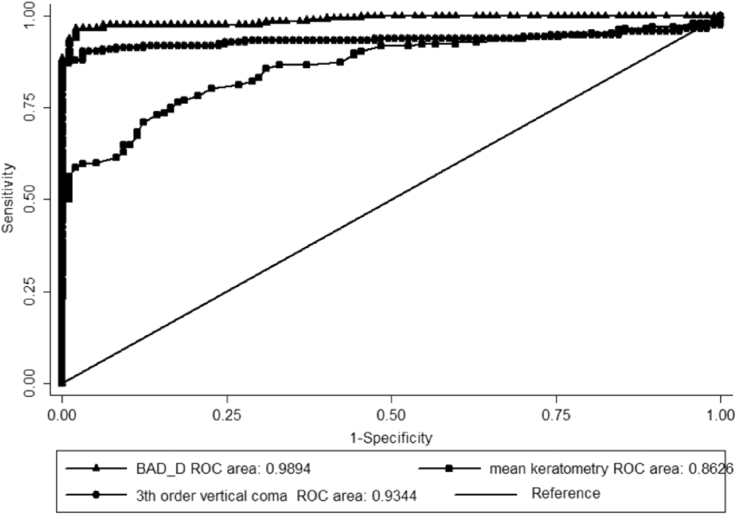
The average of all evaluated pachymetric and topometric indices and the 3rd and 5th order vertical coma aberrations showed a significant difference between the study groups (p < 0.001). Belin/Ambrosio Deviation Display (BAD_D), Index of Vertical Asymmetry (IVA), Index of Surface Variance (ISV), and 5th order vertical coma aberration were identified as the best diagnostic criteria for the diagnosis of subclinical keratoconus (R (2) = 0.65, p <0.001), and BAD_D, mean keratometry and 3rd order vertical coma aberration were identified as the best diagnostic criteria for the diagnosis of definite keratoconus (R (2) = 0.91, p <0.001). The sensitivity and specificity of the above-mentioned models were 83.6% and 96.9%, and 97.9% and 96.9%, respectively.
Simultaneous evaluation of BAD_D, 5th order vertical coma aberration, IVA, and ISV, especially when the pattern of the corneal curvature is normal, can detect subclinical keratoconus with high sensitivity and specificity. As for definite keratoconus, each of the BAD_D, mean keratometry, and 3rd order vertical coma aberration indices has a desirable diagnostic validity. However, the aforementioned indices do not negate the importance of widely recognized and acceptable indices like keratometry and central corneal thickness.
确定确诊和亚临床圆锥角膜患者的角膜厚度、像差和角膜地形图指数,以及这些指数在圆锥角膜诊断中的有效性。
本研究评估了262只圆锥角膜眼和97只健康眼。对所有参与者进行Pentacam HR检查,并提取研究人群所有角膜厚度、像差和角膜地形图指数的数据。
所有评估的角膜厚度和角膜地形图指数的平均值以及三阶和五阶垂直彗差在研究组之间存在显著差异(p<0.001)。Belin/Ambrosio偏差显示(BAD_D)、垂直不对称指数(IVA)、表面方差指数(ISV)和五阶垂直彗差被确定为亚临床圆锥角膜诊断的最佳标准(R(2)=0.65,p<0.001),BAD_D、平均角膜曲率和三阶垂直彗差被确定为确诊圆锥角膜诊断的最佳标准(R(2)=0.91,p<0.001)。上述模型的敏感性和特异性分别为83.6%和96.9%,以及97.9%和96.9%。
同时评估BAD_D、五阶垂直彗差、IVA和ISV,尤其是当角膜曲率模式正常时,可以高敏感性和特异性地检测亚临床圆锥角膜。对于确诊的圆锥角膜,BAD_D、平均角膜曲率和三阶垂直彗差指数中的每一个都具有理想的诊断有效性。然而,上述指数并不否定角膜曲率和中央角膜厚度等广泛认可和可接受的指数的重要性。