Jang Jin-Young, Heo Jin Seok, Han Youngmin, Chang Jihoon, Kim Jae Ri, Kim Hongbeom, Kwon Wooil, Kim Sun-Whe, Choi Seong Ho, Choi Dong Wook, Lee Kyoungbun, Jang Kee-Taek, Han Sung-Sik, Park Sang-Jae
From the Department of Surgery and Cancer Research Institute (J-YJ, YH, JC, JRK, HK, WK, S-WK), Seoul National University College of Medicine; Department of Surgery (JSH, WK, SHC, DWC), Sungkyunkwan University School of Medicine; Department of Pathology (KL), Seoul National University College of Medicine; Department of Pathology and Translational Genomics (K-TJ), Sungkyunkwan University School of Medicine, Seoul; and Center for Liver Cancer (S-SH, S-JP), National Cancer Center, Gyeonggido, Republic of Korea.
Medicine (Baltimore). 2016 May;95(22):e3675. doi: 10.1097/MD.0000000000003675.
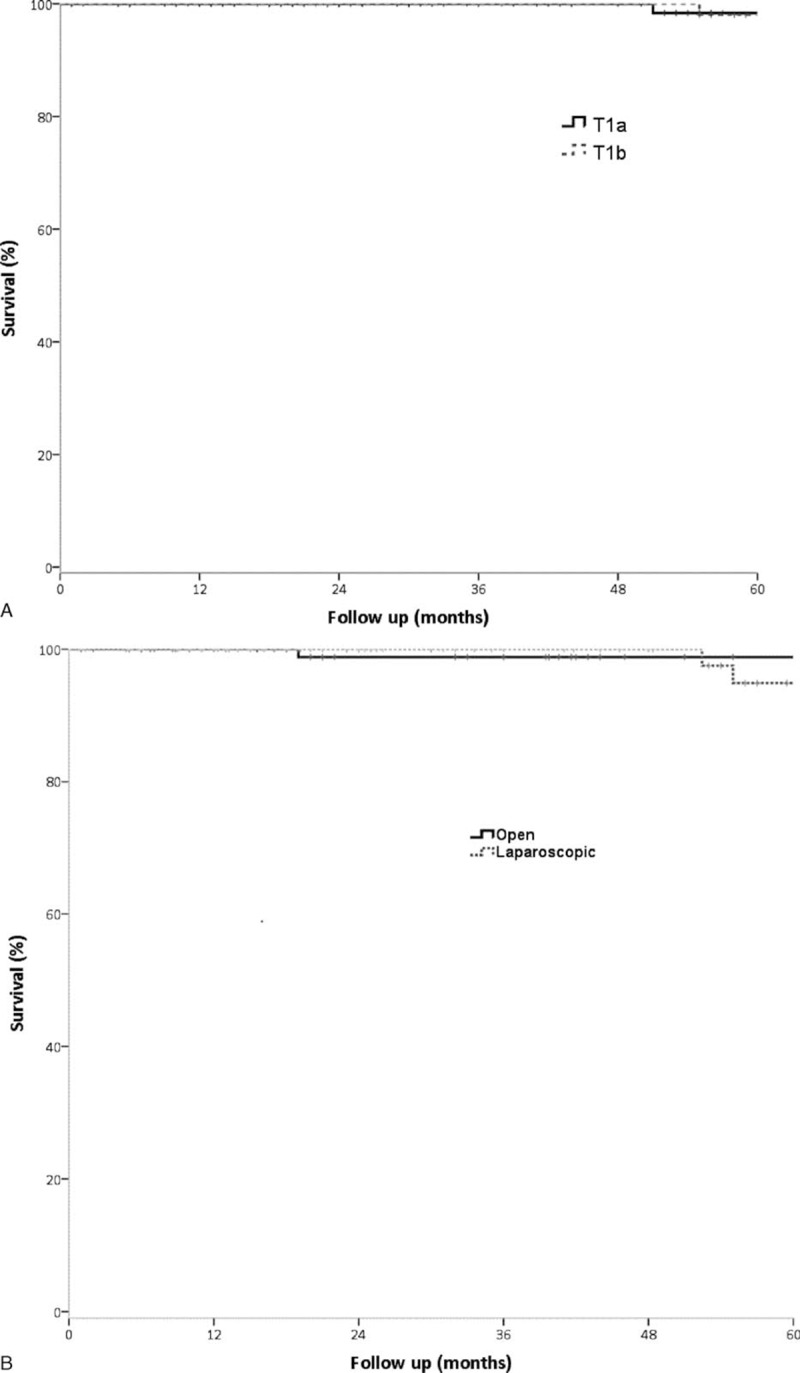
Laparoscopic surgery has been widely accepted as a feasible and safe treatment modality in many cancers of the gastrointestinal tract. However, most guidelines on gallbladder cancer (GBC) regard laparoscopic surgery as a contraindication, even for early GBC. This study aims to evaluate and compare recent surgical outcomes of laparoscopic and open surgery for T1(a,b) GBC and to determine the optimal surgical strategy for T1 GBC.The study enrolled 197 patients with histopathologically proven T1 GBC and no history of other cancers who underwent surgery from 2000 to 2014 at 3 major tertiary referral hospitals with specialized biliary-pancreas pathologists and optimal pathologic handling protocols. Median follow-up was 56 months. The effects of depth of invasion and type of surgery on disease-specific survival and recurrence patterns were investigated.Of the 197 patients, 116 (58.9%) underwent simple cholecystectomy, including 31 (15.7%) who underwent open cholecystectomy and 85 (43.1%) laparoscopic cholecystectomy. The remaining 81 (41.1%) patients underwent extended cholecystectomy. Five-year disease-specific survival rates were similar in patients who underwent simple and extended cholecystectomy (96.7% vs 100%, P = 0.483), as well as being similar in patients in the simple cholecystectomy group who underwent open and laparoscopic cholecystectomy (100% vs 97.6%, P = 0.543). Type of surgery had no effect on recurrence patterns.Laparoscopic cholecystectomy for T1 gallbladder cancer can provide similar survival outcomes compared to open surgery. Considering less blood loss and shorter hospital stay with better cosmetic outcome, laparoscopic cholecystectomy can be justified as a standard treatment for T1b as well as T1a gallbladder cancer when done by well-experienced surgeons based on exact pathologic diagnosis.
腹腔镜手术已被广泛认为是许多胃肠道癌症可行且安全的治疗方式。然而,大多数关于胆囊癌(GBC)的指南将腹腔镜手术视为禁忌,即使是早期GBC。本研究旨在评估和比较T1(a,b)期GBC腹腔镜手术和开放手术的近期手术效果,并确定T1期GBC的最佳手术策略。该研究纳入了197例经组织病理学证实为T1期GBC且无其他癌症病史的患者,这些患者于2000年至2014年在3家拥有专业胆胰病理学家和最佳病理处理方案的大型三级转诊医院接受了手术。中位随访时间为56个月。研究了浸润深度和手术类型对疾病特异性生存和复发模式的影响。197例患者中,116例(58.9%)接受了单纯胆囊切除术,其中31例(15.7%)接受了开腹胆囊切除术,85例(43.1%)接受了腹腔镜胆囊切除术。其余81例(41.1%)患者接受了扩大胆囊切除术。接受单纯胆囊切除术和扩大胆囊切除术的患者5年疾病特异性生存率相似(96.7%对100%,P = 0.483),单纯胆囊切除术中接受开腹和腹腔镜胆囊切除术的患者生存率也相似(100%对97.6%,P = 0.543)。手术类型对复发模式没有影响。对于T1期胆囊癌,腹腔镜胆囊切除术与开放手术相比可提供相似的生存结果。考虑到出血量少、住院时间短且美容效果更好,当由经验丰富的外科医生基于准确的病理诊断进行时,腹腔镜胆囊切除术可作为T1b期以及T1a期胆囊癌的标准治疗方法。