Lee Edward S, Vedanthan Rajesh, Jeemon Panniyammakal, Kamano Jemima H, Kudesia Preeti, Rajan Vikram, Engelgau Michael, Moran Andrew E
Department of Medicine, Division of Geriatric, Hospital, Palliative and General Internal Medicine, Keck School of Medicine of University of Southern California, Los Angeles, California, United States of America.
Department of Medicine, Division of Cardiology, Icahn School of Medicine at Mount Sinai, New York, New York, United States of America.
PLoS One. 2016 Jun 14;11(6):e0157036. doi: 10.1371/journal.pone.0157036. eCollection 2016.
The majority of global cardiovascular disease (CVD) burden falls on people living in low- and middle-income countries (LMICs). In order to reduce preventable CVD mortality and morbidity, LMIC health systems and health care providers need to improve the delivery and quality of CVD care.
As part of the Disease Control Priorities Three (DCP3) Study efforts addressing quality improvement, we reviewed and summarized currently available evidence on interventions to improve quality of clinic-based CVD prevention and management in LMICs.
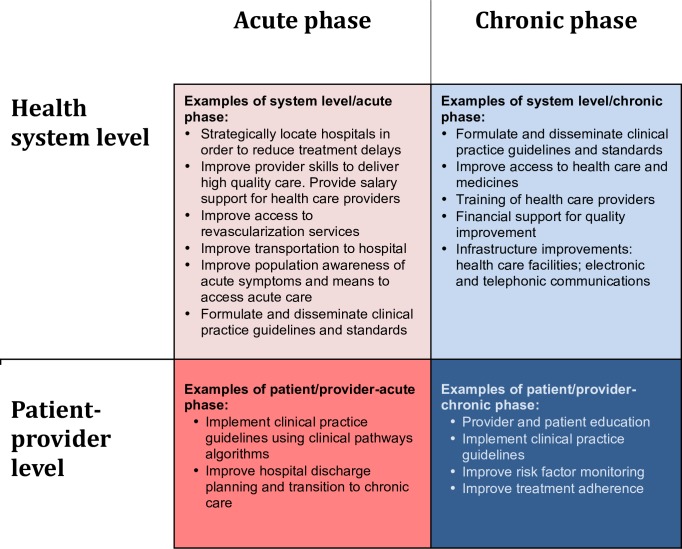
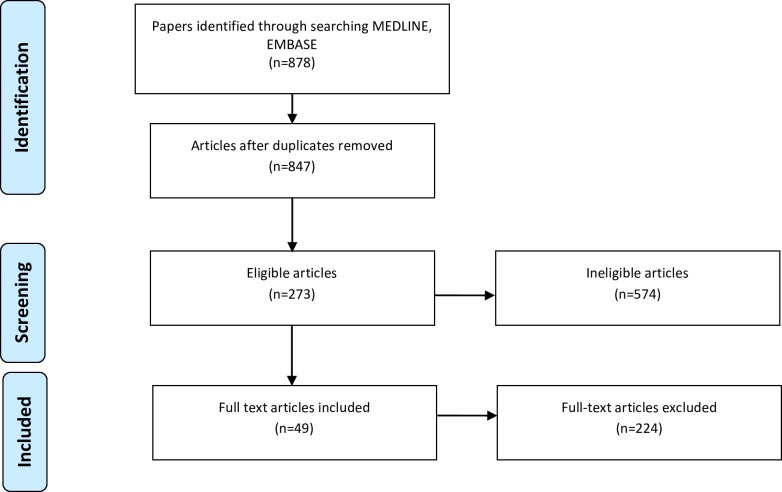
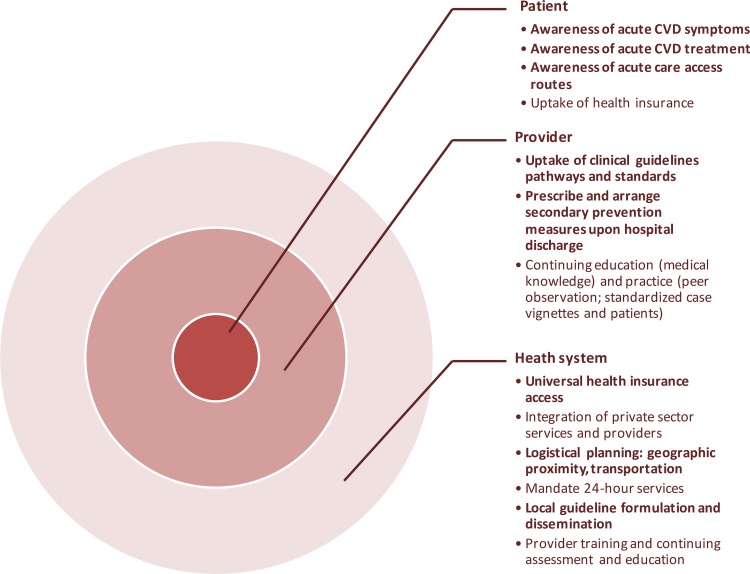
We conducted a narrative review of published comparative clinical trials that evaluated efficacy or effectiveness of clinic-based CVD prevention and management quality improvement interventions in LMICs. Conditions selected a priori included hypertension, diabetes, hyperlipidemia, coronary artery disease, stroke, rheumatic heart disease, and congestive heart failure. MEDLINE and EMBASE electronic databases were systematically searched. Studies were categorized as occurring at the system or patient/provider level and as treating the acute or chronic phase of CVD.
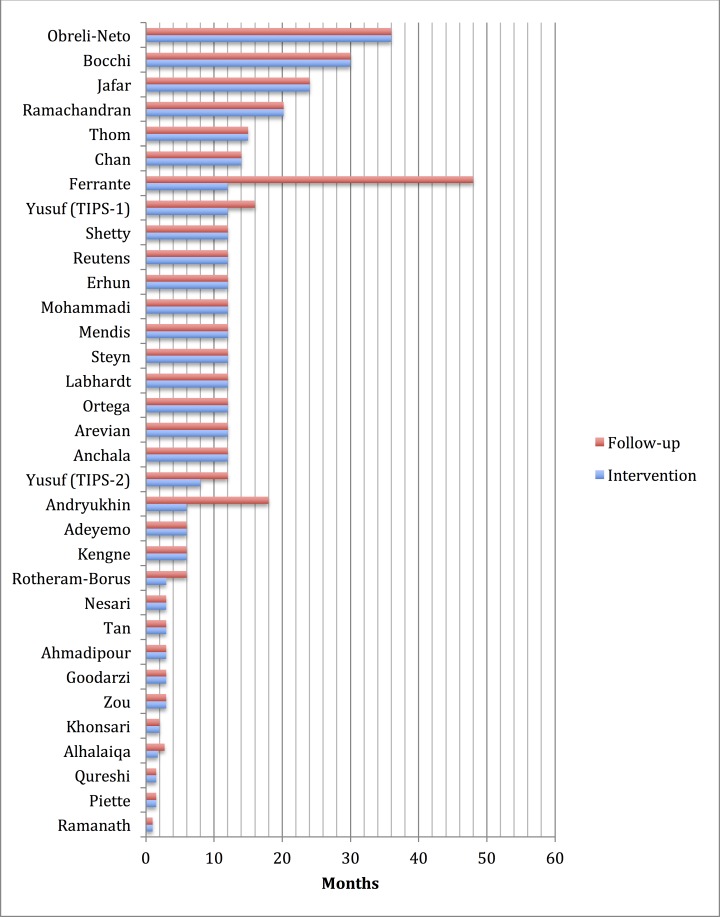
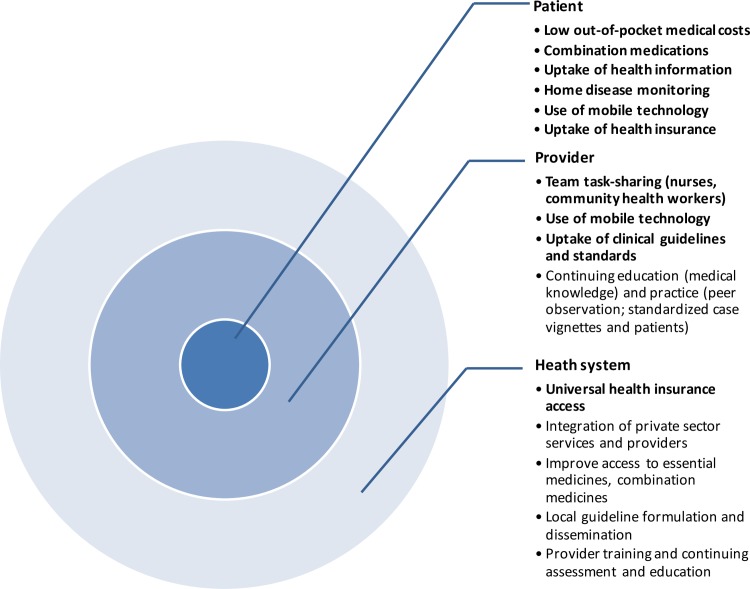
From 847 articles identified in the electronic search, 49 met full inclusion criteria and were selected for review. Selected studies were performed in 19 different LMICs. There were 10 studies of system level quality improvement interventions, 38 studies of patient/provider interventions, and one study that fit both criteria. At the patient/provider level, regardless of the specific intervention, intensified, team-based care generally led to improved medication adherence and hypertension control. At the system level, studies provided evidence that introduction of universal health insurance coverage improved hypertension and diabetes control. Studies of system and patient/provider level acute coronary syndrome quality improvement interventions yielded inconclusive results. The duration of most studies was less than 12 months.
The results of this review suggest that CVD care quality improvement can be successfully implemented in LMICs. Most studies focused on chronic CVD conditions; more acute CVD care quality improvement studies are needed. Longer term interventions and follow-up will be needed in order to assess the sustainability of quality improvement efforts in LMICs.
全球大多数心血管疾病(CVD)负担落在低收入和中等收入国家(LMICs)的人群身上。为了降低可预防的心血管疾病死亡率和发病率,LMICs的卫生系统和医疗服务提供者需要改善心血管疾病护理的提供和质量。
作为疾病控制优先事项三(DCP3)研究中解决质量改进问题的一部分,我们回顾并总结了目前关于改善LMICs中基于诊所的心血管疾病预防和管理质量的干预措施的现有证据。
我们对已发表的比较临床试验进行了叙述性综述,这些试验评估了LMICs中基于诊所的心血管疾病预防和管理质量改进干预措施的疗效或有效性。预先选定的疾病包括高血压、糖尿病、高脂血症、冠状动脉疾病、中风、风湿性心脏病和充血性心力衰竭。系统检索了MEDLINE和EMBASE电子数据库。研究被分类为发生在系统或患者/提供者层面,以及治疗心血管疾病的急性期或慢性期。
在电子检索中识别出的847篇文章中,49篇符合完全纳入标准并被选入综述。选定的研究在19个不同的LMICs中进行。有10项关于系统层面质量改进干预措施的研究,38项关于患者/提供者干预措施的研究,以及1项符合两项标准的研究。在患者/提供者层面,无论具体干预措施如何,强化的、基于团队的护理通常会导致药物依从性和高血压控制得到改善。在系统层面,研究提供的证据表明,引入全民健康保险覆盖改善了高血压和糖尿病的控制。关于系统和患者/提供者层面急性冠状动脉综合征质量改进干预措施的研究结果尚无定论。大多数研究的持续时间不到12个月。
本综述结果表明,心血管疾病护理质量改进可以在LMICs中成功实施。大多数研究集中在慢性心血管疾病方面;需要更多关于急性心血管疾病护理质量改进的研究。为了评估LMICs中质量改进努力的可持续性,将需要长期干预和随访。