Park Jin-Seok, Kim Min Su, Kim HyungKil, Kim Shin Il, Shin Chun Ho, Lee Hyun Jung, Lee Won Seop, Moon Soyoung
Digestive Disease Center, Department of Internal Medicine, Inha University School of Medicine, 27 Inhang-ro, Jung-gu, Incheon, 400-711, South Korea.
BMC Gastroenterol. 2016 Jun 17;16(1):64. doi: 10.1186/s12876-016-0476-6.
High-quality bowel preparation is necessary for colonoscopy. A few studies have been conducted to investigate improvement in bowel preparation quality through patient education. However, the effect of patient education on bowel preparation has not been well studied.
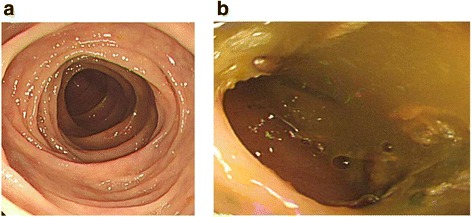
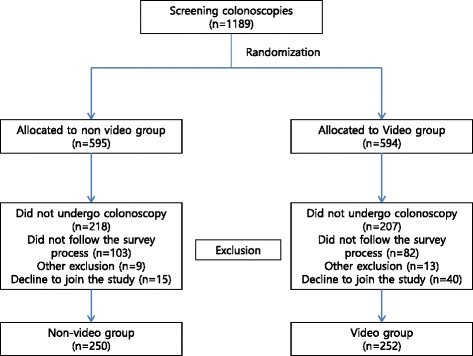
A randomized and prospective study was conducted. All patients received regular instruction for bowel preparation during a pre-colonoscopy visit. Those scheduled for colonoscopy were randomly assigned to view an educational video instruction (video group) on the day before the colonoscopy, or to a non-video (control) group. Qualities of bowel preparation using the Ottawa Bowel Preparation Quality scale (Ottawa score) were compared between the video and non-video groups. In addition, factors associated with poor bowel preparation were investigated.
A total of 502 patients were randomized, 250 to the video group and 252 to the non-video group. The video group exhibited better bowel preparation (mean Ottawa total score: 3.03 ± 1.9) than the non-video group (4.21 ± 1.9; P < 0.001) and had good bowel preparation for colonoscopy (total Ottawa score <6: 91.6 % vs. 78.5 %; P < 0.001). Multivariate analysis revealed that males (odds ratio [OR] = 1.95, P = 0.029), diabetes mellitus patients (OR = 2.79, P = 0.021), and non-use of visual aids (OR = 3.09, P < 0.001) were associated with poor bowel preparation. In the comparison of the colonoscopic outcomes between groups, the polyp detection rate was not significantly different between video group and non-video group (48/250, 19.2 % vs. 48/252, 19.0 %; P = 0.963), but insertion time was significantly short in video group (5.5 ± 3.2 min) than non-video group (6.1 ± 3.7 min; P = 0.043).
The addition of an educational video could improve the quality of bowel preparation in comparison with standard preparation method.
Clinical Research Information Service KCT0001836 . The date of registration: March, 08(th), 2016, Retrospectively registered.
高质量的肠道准备对于结肠镜检查是必要的。已经开展了一些研究来调查通过患者教育改善肠道准备质量的情况。然而,患者教育对肠道准备的影响尚未得到充分研究。
进行了一项随机前瞻性研究。所有患者在结肠镜检查前的就诊期间接受常规的肠道准备指导。计划进行结肠镜检查的患者被随机分为在结肠镜检查前一天观看教育视频指导(视频组)或非视频(对照组)组。使用渥太华肠道准备质量量表(渥太华评分)比较视频组和非视频组的肠道准备质量。此外,还调查了与肠道准备不佳相关的因素。
总共502例患者被随机分组,250例进入视频组,252例进入非视频组。视频组的肠道准备情况(渥太华总分均值:3.03±1.9)优于非视频组(4.21±1.9;P<0.001),并且结肠镜检查的肠道准备良好(渥太华总分<6:91.6%对78.5%;P<0.001)。多因素分析显示,男性(优势比[OR]=1.95,P=0.029)、糖尿病患者(OR=2.79,P=0.021)和未使用视觉辅助工具(OR=3.09,P<0.001)与肠道准备不佳相关。在比较两组的结肠镜检查结果时,视频组和非视频组的息肉检出率无显著差异(48/250,19.2%对48/252,19.0%;P=0.963),但视频组的插入时间(5.5±3.2分钟)显著短于非视频组(6.1±3.7分钟;P=0.043)。
与标准准备方法相比,增加教育视频可改善肠道准备质量。
临床研究信息服务KCT0001836。注册日期:2016年3月8日,回顾性注册。