Zittermann Armin, Kuhn Joachim, Ernst Jana B, Becker Tobias, Larisch Julia, Dreier Jens, Knabbe Cornelius, Börgermann Jochen, Gummert Jan F
Clinic for Thoracic and Cardiovascular Surgery, Heart and Diabetes Center North Rhine-Westphalia, Ruhr University Bochum, Bad Oeynhausen, Germany.
Institute for Laboratory and Transfusion Medicine, Heart and Diabetes Center North Rhine-Westphalia, Ruhr University Bochum, Bad Oeynhausen, Germany.
PLoS One. 2016 Jun 29;11(6):e0158532. doi: 10.1371/journal.pone.0158532. eCollection 2016.
Vitamin D has immunomodulatory properties and seems to reduce the risk of infections. Whether low vitamin D concentrations are independent risk factors for nosocomial postoperative infections in surgical patients remains to be studied in detail.
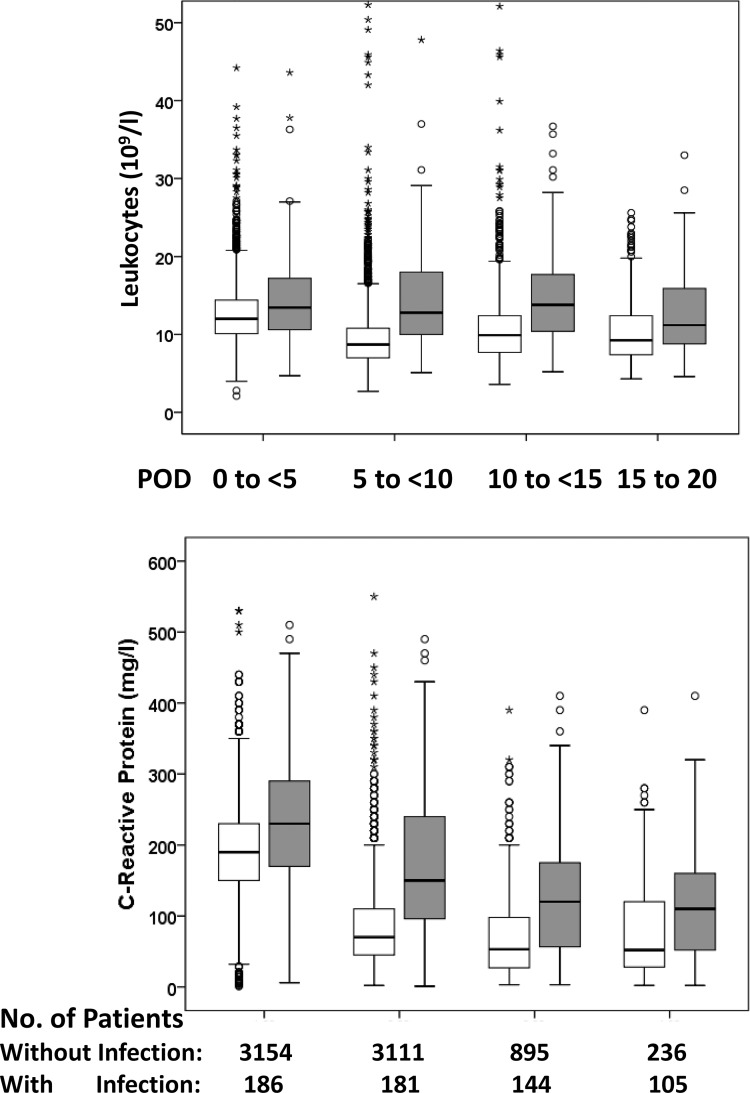
In 3,340 consecutive cardiac surgical patients, we investigated the association of circulating 25-hydroxyvitamin D (25OHD; indicator of nutritional vitamin D status) and 1,25-dihydroxyvitamin D (1,25[OH]2D; active vitamin D hormone) with nosocomicial infections. The primary endpoint was a composite of thoracic wound infection, sepsis, and broncho-pulmonary infection. Vitamin D status was measured on the last preoperative day. Infections were assessed until discharge. Logistic regression analysis was used to examine the association between vitamin D metabolite concentrations and the composite endpoint.
The primary endpoint was reached by 5.6% (n = 186). In patients who reached and did not reach the endpoint, in-hospital mortality was 13.4% and 1.5%, respectively (P<0.001). Median (IQR) 25OHD and 1,25(OH)2D concentrations were 43. 2 (29.7-61.9) nmol/l and 58.0 (38.5-77.5) pmol/l, respectively. Compared with the highest 1,25(OH)2D quintile (>81.0 pmol/l), the multivariable-adjusted odds ratio of infection was 2.57 (95%CI:1.47-4.49) for the lowest 1,25(OH)2D quintile (<31.5 pmol/l) and 1.85 (95%CI:1.05-3.25) for the second lowest quintile (31.5-49.0 pmol/l). There was no significant association between 25OHD concentrations and the primary endpoint.
Our data indicate an independent association of low 1,25(OH)2D levels with the risk of postoperative infections in cardiac surgical patients. Future studies should pay more attention on the clinical relevance of circulating 1,25(OH)2D and its regulation.
维生素D具有免疫调节特性,似乎能降低感染风险。维生素D浓度低是否是外科手术患者医院获得性术后感染的独立危险因素,仍有待详细研究。
在3340例连续的心脏外科手术患者中,我们研究了循环25-羟基维生素D(25OHD;营养性维生素D状态指标)和1,25-二羟基维生素D(1,25[OH]2D;活性维生素D激素)与医院获得性感染之间的关联。主要终点是胸壁伤口感染、脓毒症和支气管肺部感染的综合指标。在术前最后一天测量维生素D状态。对感染情况进行评估直至出院。采用逻辑回归分析来检验维生素D代谢物浓度与综合终点之间的关联。
5.6%(n = 186)的患者达到主要终点。达到和未达到终点的患者,住院死亡率分别为13.4%和1.5%(P<0.001)。25OHD和1,25(OH)2D浓度的中位数(四分位间距)分别为43.2(29.7 - 61.9)nmol/l和58.0(38.5 - 77.5)pmol/l。与1,25(OH)2D最高五分位数(>81.0 pmol/l)相比,1,25(OH)2D最低五分位数(<31.5 pmol/l)感染的多变量调整比值比为2.57(95%置信区间:1.47 - 4.49),第二低五分位数(31.5 - 49.0 pmol/l)为1.85(95%置信区间:1.05 - 3.25)。25OHD浓度与主要终点之间无显著关联。
我们的数据表明,低1,25(OH)2D水平与心脏外科手术患者术后感染风险存在独立关联。未来的研究应更多关注循环1,25(OH)2D的临床相关性及其调节。