Zarski Anna-Carlotta, Lehr Dirk, Berking Matthias, Riper Heleen, Cuijpers Pim, Ebert David Daniel
Department of Clinical Psychology and Psychotherapy, Friedrich-Alexander University Erlangen-Nuremberg, Erlangen, Germany.
J Med Internet Res. 2016 Jun 29;18(6):e146. doi: 10.2196/jmir.4493.
Nonadherence to treatment is a prevalent issue in Internet interventions. Guidance from health care professionals has been found to increase treatment adherence rates in Internet interventions for a range of physical and mental disorders. Evaluating different guidance formats of varying intensity is important, particularly with respect to improvement of effectiveness and cost-effectiveness. Identifying predictors of nonadherence allows for the opportunity to better adapt Internet interventions to the needs of participants especially at risk for discontinuing treatment.
The goal of this study was to investigate the influence of different guidance formats (content-focused guidance, adherence-focused guidance, and administrative guidance) on adherence and to identify predictors of nonadherence in an Internet-based mobile-supported stress management intervention (ie, GET.ON Stress) for employees.
The data from the groups who received the intervention were pooled from three randomized controlled trials (RCTs) that evaluated the efficacy of the same Internet-based mobile-supported stress management intervention (N=395). The RCTs only differed in terms of the guidance format (content-focused guidance vs waitlist control, adherence-focused guidance vs waitlist control, administrative guidance vs waitlist control). Adherence was defined by the number of completed treatment modules (0-7). An ANOVA was performed to compare the adherence rates from the different guidance formats. Multiple hierarchical linear regression analysis was conducted to evaluate predictors of nonadherence, which included gender, age, education, symptom-related factors, and hope for improvement.
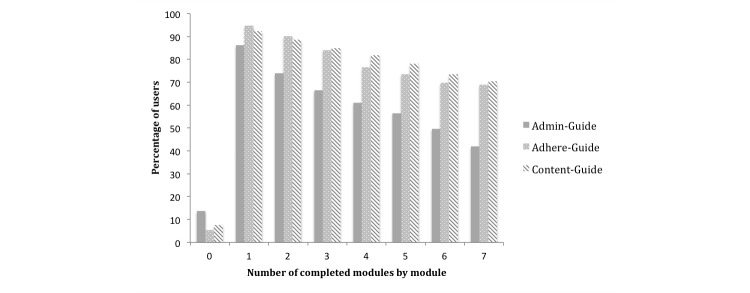
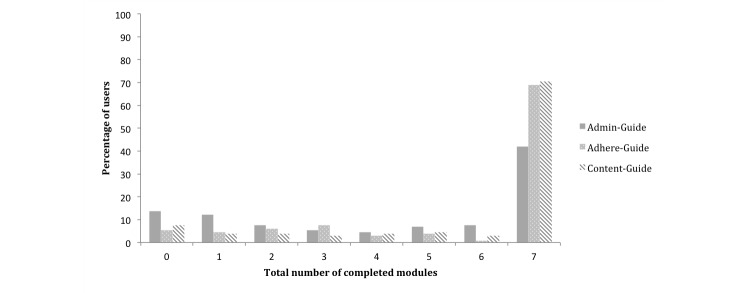
In all, 70.5% (93/132) of the content-focused guidance sample, 68.9% (91/132) of the adherence-focused guidance sample, and 42.0% (55/131) of the participants in the administrative guidance sample completed all treatment modules. Guidance had a significant effect on treatment adherence (F2,392=11.64, P<.001; ω(2)=.05). Participants in the content-focused guidance (mean 5.70, SD 2.32) and adherence-focused guidance samples (mean 5.58, SD 2.33) completed significantly more modules than participants in the administrative guidance sample (mean 4.36, SD 2.78; t223=4.53, P<.001; r=.29). Content-focused guidance was not significantly associated with higher adherence compared to adherence-focused guidance (t262=0.42, P=.67; r=.03). The effect size of r=.03 (95% CI -0.09 to 0.15) did not pass the equivalence margin of r=.20 and the upper bound of the 95% CI lay below the predefined margin, indicating equivalence between adherence-focused guidance and content-focused guidance. Beyond the influence of guidance, none of the predictors significantly predicted nonadherence.
Guidance has been shown to be an influential factor in promoting adherence to an Internet-based mobile-supported stress management intervention. Adherence-focused guidance, which included email reminders and feedback on demand, was equivalent to content-focused guidance with regular feedback while requiring only approximately a quarter of the coaching resources. This could be a promising discovery in terms of cost-effectiveness. However, even after considering guidance, sociodemographic, and symptom-related characteristics, most interindividual differences in nonadherence remain unexplained.
DRKS00004749; http://drks-neu.uniklinik-freiburg.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL _ID=DRKS00004749 (Archived by WebCite at http://www.webcitation.org/6QiDk9Zn8); DRKS00005112; http://drks-neu.uniklinik-freiburg. de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005112 (Archived by WebCite at http://www.webcitation.org/6QiDysvev); DRKS00005384; http://drks-neu.uniklinik-freiburg.de/ drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005384 (Archived by WebCite at http://www.webcitation.org/6QiE0xcpE).
治疗依从性不佳是互联网干预中的一个普遍问题。研究发现,医疗保健专业人员的指导能够提高针对一系列身心疾病的互联网干预中的治疗依从率。评估不同强度的指导形式非常重要,特别是在提高有效性和成本效益方面。识别不依从的预测因素有助于更好地使互联网干预适应参与者的需求,尤其是那些有中断治疗风险的参与者。
本研究的目的是调查不同指导形式(内容聚焦指导、依从性聚焦指导和行政指导)对依从性的影响,并识别基于互联网的移动支持压力管理干预(即GET.ON Stress)中员工不依从的预测因素。
接受干预的组的数据来自三项随机对照试验(RCT),这些试验评估了相同的基于互联网的移动支持压力管理干预的疗效(N = 395)。这些RCT仅在指导形式上有所不同(内容聚焦指导与等待列表对照、依从性聚焦指导与等待列表对照、行政指导与等待列表对照)。依从性通过完成的治疗模块数量(0 - 7)来定义。进行方差分析以比较不同指导形式的依从率。进行多元分层线性回归分析以评估不依从的预测因素,包括性别、年龄、教育程度、症状相关因素和改善的希望。
总体而言,内容聚焦指导样本中的70.5%(93/132)、依从性聚焦指导样本中的68.9%(91/132)以及行政指导样本中的42.0%(55/131)的参与者完成了所有治疗模块。指导对治疗依从性有显著影响(F2,392 = 11.64,P <.001;ω(2)=.05)。内容聚焦指导样本(均值5.70,标准差2.32)和依从性聚焦指导样本(均值5.58,标准差2.33)中的参与者完成了比行政指导样本(均值4.36,标准差2.78)中的参与者显著更多的模块(t223 = 4.53,P <.001;r =.29)。与依从性聚焦指导相比,内容聚焦指导与更高的依从性没有显著关联(t262 = 0.42,P =.67;r =.03)。r =.03(95% CI -0.09至0.1十五)的效应大小未超过r =.20的等效边界,且95% CI的上限低于预定义边界,表明依从性聚焦指导和内容聚焦指导之间等效。除了指导的影响外,没有一个预测因素能显著预测不依从。
指导已被证明是促进基于互联网的移动支持压力管理干预依从性的一个有影响的因素。包括电子邮件提醒和按需反馈的依从性聚焦指导与具有定期反馈的内容聚焦指导等效,同时仅需要大约四分之一的指导资源。就成本效益而言,这可能是一个有前景的发现。然而,即使考虑了指导、社会人口统计学和症状相关特征,大多数不依从的个体间差异仍无法解释。
DRKS00004749;http://drks - neu.uniklinik - freiburg.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL _ID=DRKS00004749(由WebCite存档于http://www.webcitation.org/6QiDk9Zn8);DRKS00005112;http://drks - neu.uniklinik - freiburg. de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005112(由WebCite存档于http://www.webcitation.org/6QiDysvev);DRKS00005384;http://drks - neu.uniklinik - freiburg.de/ drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00005384(由WebCite存档于http://www.webcitation.org/6QiE0xcpE)。