Hontelez Jan A C, Tanser Frank C, Naidu Kevindra K, Pillay Deenan, Bärnighausen Till
Wellcome Trust Africa Centre for Population Health, University of KwaZulu-Natal, Mtubatuba, South Africa.
Department of Global Health and Population, Harvard T.H. Chan School of Public Health, Boston, United States of America.
PLoS One. 2016 Jul 6;11(7):e0158015. doi: 10.1371/journal.pone.0158015. eCollection 2016.
The effect of the rapid scale-up of vertical antiretroviral treatment (ART) programs for HIV in sub-Saharan Africa on the overall health system is under intense debate. Some have argued that these programs have reduced access for people suffering from diseases unrelated to HIV because ART programs have drained human and physical resources from other parts of the health system; others have claimed that the investments through ART programs have strengthened the general health system and the population health impacts of ART have freed up health care capacity for the treatment of diseases that are not related to HIV. To establish the population-level impact of ART programs on health care utilization in the public-sector health system, we compared trends in health care utilization among HIV-infected people receiving and not receiving ART with HIV-uninfected people during a period of rapid ART scale-up.
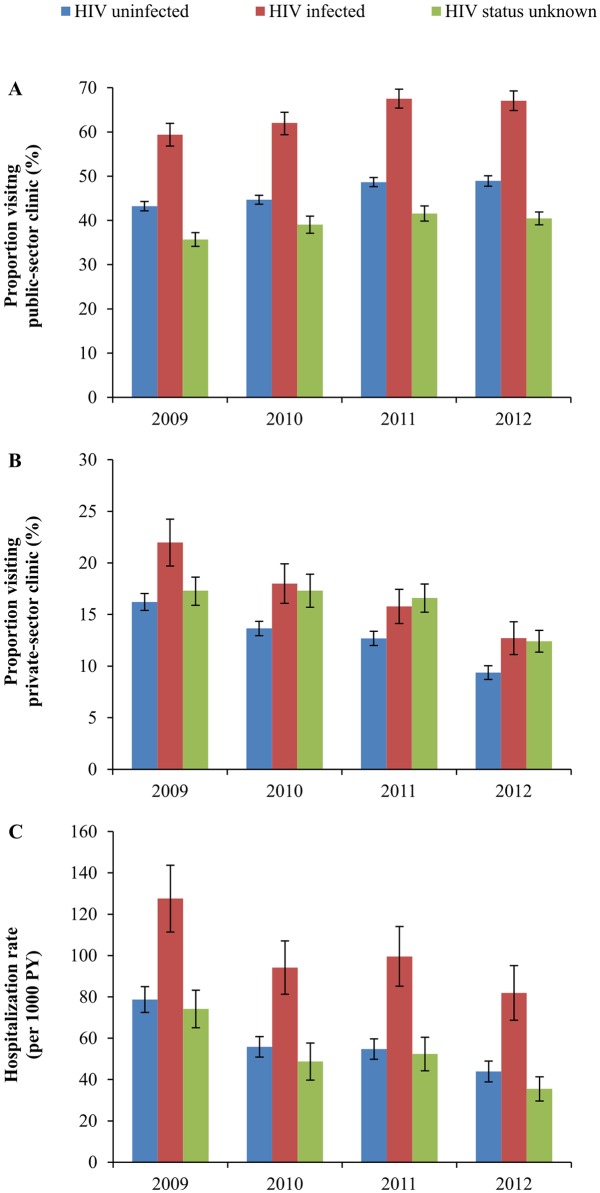
We used data from the Wellcome Trust Africa Centre for Population Health, which annually elicited information on health care utilization from all surveillance participants over the period 2009-2012 (N = 32,319). We determined trends in hospitalization, and public-sector and private-sector primary health care (PHC) clinic visits for HIV-infected and -uninfected people over a time period of rapid ART scale-up (2009-2012) in this community. We regressed health care utilization on HIV status and ART status in different calendar years, controlling for sex, age, and area of residence. The proportion of people who reported to have visited a public-sector primary health care (PHC) clinic in the last 6 months increased significantly over the period 2009-2012, for both HIV-infected people (from 59% to 67%; p<0.001), and HIV-uninfected people (from 41% to 47%; p<0.001). In contrast, the proportion of HIV-infected people visiting a private-sector PHC clinic declined from 22% to 12% (p<0.001) and hospitalization rates declined from 128 to 82 per 1000 PY (p<0.001). For HIV-uninfected people, the proportion visiting a private-sector PHC clinic declined from 16% to 9%, and hospitalization rates declined from 78 to 44 per 1000 PY (p<0.001). After controlling for potential confounding factors, all trends remained of similar magnitude and significance.
Our results indicate that the ART scale-up in this high HIV prevalence community has shifted health care utilization from hospitals and private-sector primary care to public-sector primary care. Remarkably, this shift is observed for both HIV-infected and -uninfected populations, supporting and extending hypotheses of 'therapeutic citizenship' whereby HIV-infected patients receiving ART facilitate primary care access for family and community members. One explanation of our findings is that ART has improved the capacity or quality of primary care in this community and, as a consequence, increasingly met overall health care needs at the primary care level rather than at the secondary level. Future research needs to confirm this causal interpretation of our findings using qualitative work to understand causal mechanisms or quasi-experimental quantitative studies to increase the strength of causal inference.
撒哈拉以南非洲地区针对艾滋病病毒(HIV)的垂直抗逆转录病毒治疗(ART)项目迅速扩大,其对整个卫生系统的影响正引发激烈辩论。一些人认为,这些项目减少了与HIV无关疾病患者的就医机会,因为ART项目耗尽了卫生系统其他部门的人力和物力资源;另一些人则称,通过ART项目的投资加强了整体卫生系统,且ART对人群健康的影响释放了医疗保健能力,可用于治疗与HIV无关的疾病。为确定ART项目在公共部门卫生系统中对医疗保健利用的人群层面影响,我们比较了在ART迅速扩大期间,接受和未接受ART的HIV感染者与未感染HIV者在医疗保健利用方面的趋势。
我们使用了威康信托非洲人口健康中心的数据,该中心在2009年至2012年期间每年收集所有监测参与者的医疗保健利用信息(N = 32319)。我们确定了在该社区ART迅速扩大期间(2009年至2012年),HIV感染者和未感染者住院以及在公共部门和私营部门初级卫生保健(PHC)诊所就诊的趋势。我们对不同日历年份的HIV状态和ART状态与医疗保健利用进行回归分析,同时控制性别、年龄和居住地区。在2009年至2012年期间,过去6个月内报告去过公共部门初级卫生保健(PHC)诊所的人群比例显著增加,HIV感染者(从59%增至67%;p<0.001)和未感染HIV者(从41%增至47%;p<0.001)均是如此。相比之下,HIV感染者前往私营部门PHC诊所就诊的比例从22%降至12%(p<0.001),住院率从每1000人年128例降至82例(p<0.001)。对于未感染HIV者,前往私营部门PHC诊所就诊的比例从16%降至9%,住院率从每1000人年78例降至44例(p<0.001)。在控制潜在混杂因素后,所有趋势的幅度和显著性仍相似。
我们的结果表明,在这个HIV高流行社区扩大ART规模已使医疗保健利用从医院和私营部门初级保健转向公共部门初级保健。值得注意的是,在HIV感染者和未感染者中均观察到这种转变,支持并扩展了“治疗公民身份”的假设,即接受ART的HIV感染患者为家人和社区成员获得初级保健提供了便利。对我们研究结果的一种解释是,ART提高了该社区初级保健的能力或质量,因此越来越多地在初级保健层面而非二级保健层面满足整体医疗保健需求。未来的研究需要使用定性研究来理解因果机制,或通过准实验定量研究来加强因果推断,以证实我们研究结果的这种因果解释。