Fraccaro Paolo, van der Veer Sabine, Brown Benjamin, Prosperi Mattia, O'Donoghue Donal, Collins Gary S, Buchan Iain, Peek Niels
NIHR Greater Manchester Primary Care Patient Safety Translational Research Centre, Institute of Population Health, The University of Manchester, Manchester, UK.
Health eResearch Centre, Farr Institute for Health Informatics Research, Manchester, UK.
BMC Med. 2016 Jul 12;14:104. doi: 10.1186/s12916-016-0650-2.
Chronic kidney disease (CKD) is a major and increasing constituent of disease burdens worldwide. Early identification of patients at increased risk of developing CKD can guide interventions to slow disease progression, initiate timely referral to appropriate kidney care services, and support targeting of care resources. Risk prediction models can extend laboratory-based CKD screening to earlier stages of disease; however, to date, only a few of them have been externally validated or directly compared outside development populations. Our objective was to validate published CKD prediction models applicable in primary care.
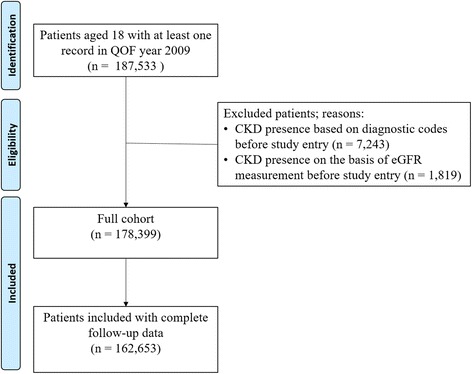
We synthesised two recent systematic reviews of CKD risk prediction models and externally validated selected models for a 5-year horizon of disease onset. We used linked, anonymised, structured (coded) primary and secondary care data from patients resident in Salford (population ~234 k), UK. All adult patients with at least one record in 2009 were followed-up until the end of 2014, death, or CKD onset (n = 178,399). CKD onset was defined as repeated impaired eGFR measures over a period of at least 3 months, or physician diagnosis of CKD Stage 3-5. For each model, we assessed discrimination, calibration, and decision curve analysis.
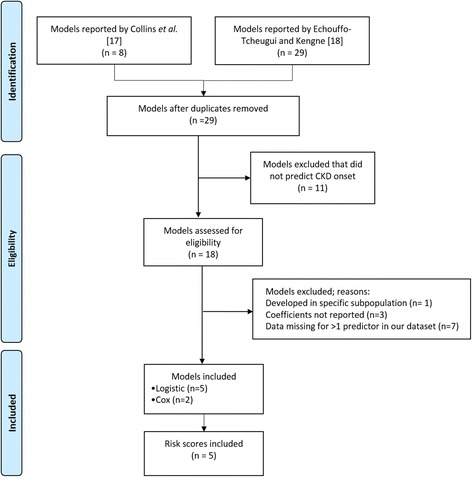
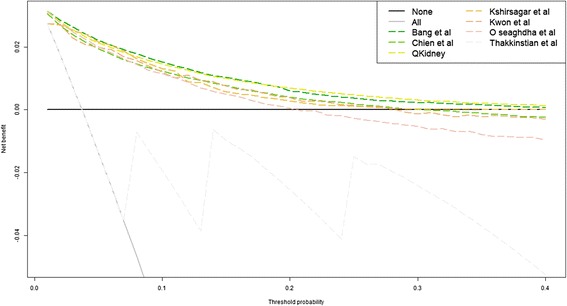
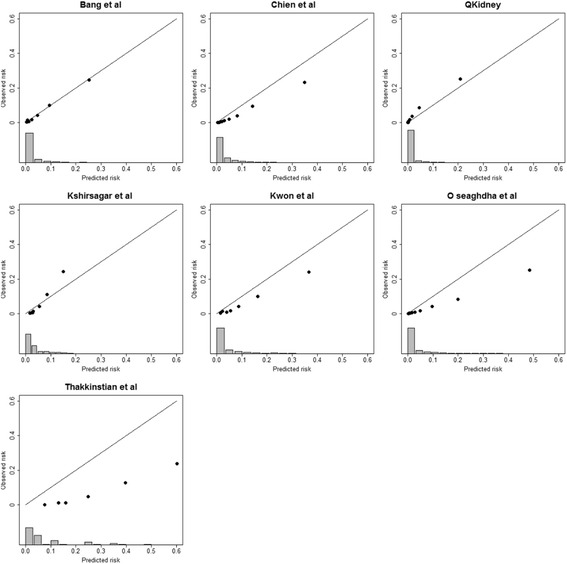
Seven relevant CKD risk prediction models were identified. Five models also had an associated simplified scoring system. All models discriminated well between patients developing CKD or not, with c-statistics around 0.90. Most of the models were poorly calibrated to our population, substantially over-predicting risk. The two models that did not require recalibration were also the ones that had the best performance in the decision curve analysis.
Included CKD prediction models showed good discriminative ability but over-predicted the actual 5-year CKD risk in English primary care patients. QKidney, the only UK-developed model, outperformed the others. Clinical prediction models should be (re)calibrated for their intended uses.
慢性肾脏病(CKD)是全球疾病负担中一个主要且不断增加的组成部分。早期识别有患CKD风险增加的患者,可指导采取干预措施以减缓疾病进展,及时转诊至合适的肾脏护理服务机构,并支持对护理资源的合理分配。风险预测模型可将基于实验室的CKD筛查扩展至疾病的更早阶段;然而,迄今为止,只有少数模型在外部得到验证或在开发人群之外进行过直接比较。我们的目的是验证适用于初级保健的已发表的CKD预测模型。
我们综合了两项近期关于CKD风险预测模型的系统评价,并对选定模型进行了外部验证,以预测5年的疾病发病情况。我们使用了来自英国索尔福德(人口约23.4万)居民的关联、匿名、结构化(编码)的初级和二级保健数据。所有在2009年至少有一条记录的成年患者均随访至2014年底、死亡或CKD发病(n = 178,399)。CKD发病定义为在至少3个月的时间内多次估算肾小球滤过率(eGFR)测量值受损,或医生诊断为CKD 3 - 5期。对于每个模型,我们评估了区分度、校准度和决策曲线分析。
共识别出7个相关的CKD风险预测模型。5个模型还伴有简化评分系统。所有模型在区分发生CKD的患者和未发生CKD的患者方面表现良好,c统计量约为0.90。大多数模型与我们的研究人群校准度不佳,对风险的预测大幅高估。两个无需重新校准的模型在决策曲线分析中也表现最佳。
纳入的CKD预测模型显示出良好的区分能力,但高估了英国初级保健患者实际的5年CKD风险。英国唯一开发的模型QKidney表现优于其他模型。临床预测模型应针对其预期用途进行(重新)校准。