You Wendong, Feng Junfeng, Tang Qilin, Cao Jun, Wang Lei, Lei Jin, Mao Qing, Gao Guoyi, Jiang Jiyao
Department of Neurosurgery, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200127, People's Republic of China.
Shanghai Institute of Head Trauma, Shanghai, 200127, People's Republic of China.
BMC Anesthesiol. 2016 Jul 11;16(1):35. doi: 10.1186/s12871-016-0199-9.
Intracranial pressure (ICP) monitoring is widely used in the management of patients with severe traumatic brain injury (TBI). However, there is limited evidence about the efficacy of ICP monitoring in older subjects (aged ≥65 years). This study evaluated the effect of intraventricular ICP monitoring on the outcome of older adults suffering from a severe TBI.
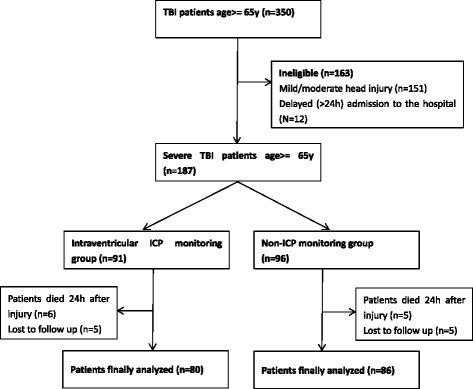
This prospective, observational study included 166 older TBI patients (aged ≥65 years) with Glasgow Coma scale (GCS) scores lower than 9 at admission. The study cohort was divided into two groups, intraventricular ICP monitoring and non-ICP monitoring. The primary outcome was in-hospital mortality. The secondary outcomes included the Glasgow Outcome Scale (GOS) score 6 months after injury, the ICU and total hospital lengths of stay, and mechanical ventilation days.
There were 80 patients in the intraventricular ICP monitoring group and 86 patients in non-ICP monitoring group. There was no statistical difference between groups in demographics and severity of head injury. Patients treated with intraventricular ICP monitoring had lower in-hospital mortality (33.8 % vs 51.2 %, P < 0.05), a higher 6-month GOS score (3.0 ± 1.4 vs 2.5 ± 1.2 P < 0.05), and a lower dosage (514 ± 246 g vs 840 ± 323 g, P < 0.0001) and shorter duration (7.2 ± 3.6 days vs 8.4 ± 4.3 days, P < 0.01) of mannitol use. However, the ICU length of stay (14.3 ± 6.4 days vs 11.6 ± 5.8 days, P < 0.01) and mechanical ventilation days (6.7 ± 3.5 days vs 5.6 ± 2.4 days, P < 0.05) were longer in the ICP monitoring group. The total length of hospital stay did not differ between the two groups (28.5 ± 12.1 days vs 26.1 ± 13.5 days, P = 0.23).
Intraventricular ICP monitoring may have beneficial effects on the decreased in-hospital mortality and improved 6-month outcome of older patients with severe TBI. However, given that this was an observational study conducted in a single institution, further well-designed randomized control trials are needed to evaluate the effect of intraventricular ICP monitoring on the outcome of older severe TBI patients.
颅内压(ICP)监测广泛应用于重度创伤性脑损伤(TBI)患者的治疗中。然而,关于ICP监测在老年患者(年龄≥65岁)中的疗效证据有限。本研究评估了脑室内ICP监测对重度TBI老年患者预后的影响。
这项前瞻性观察性研究纳入了166例老年TBI患者(年龄≥65岁),入院时格拉斯哥昏迷量表(GCS)评分低于9分。研究队列分为两组,即脑室内ICP监测组和非ICP监测组。主要结局是院内死亡率。次要结局包括伤后6个月的格拉斯哥预后量表(GOS)评分、ICU住院时间和总住院时间以及机械通气天数。
脑室内ICP监测组有80例患者,非ICP监测组有86例患者。两组在人口统计学和颅脑损伤严重程度方面无统计学差异。接受脑室内ICP监测治疗的患者院内死亡率较低(33.8%对51.2%,P<0.05),伤后6个月GOS评分较高(3.0±1.4对2.5±1.2,P<0.05),甘露醇使用剂量较低(514±246克对840±323克,P<0.0001)且使用时间较短(7.2±3.6天对8.4±4.3天,P<0.01)。然而,ICP监测组的ICU住院时间(14.3±6.4天对11.6±5.8天,P<0.01)和机械通气天数(6.7±3.5天对5.6±2.4天,P<0.05)更长。两组的总住院时间无差异(28.5±12.1天对26.1±13.5天,P=0.23)。
脑室内ICP监测可能对降低重度TBI老年患者的院内死亡率和改善其伤后6个月的预后有有益影响。然而,鉴于这是在单一机构进行的观察性研究,需要进一步设计完善的随机对照试验来评估脑室内ICP监测对重度TBI老年患者预后的影响。