2nd Department of Intensive Care Medicine, George Papanikolaou General Hospital, G. Papanikolaou Avenue, 57010, Exochi, Thessaloniki, Greece.
1st Department of Intensive Care Medicine, George Papanikolaou General Hospital, Thessaloniki, Greece.
J Anesth. 2020 Oct;34(5):741-757. doi: 10.1007/s00540-020-02795-7. Epub 2020 May 21.
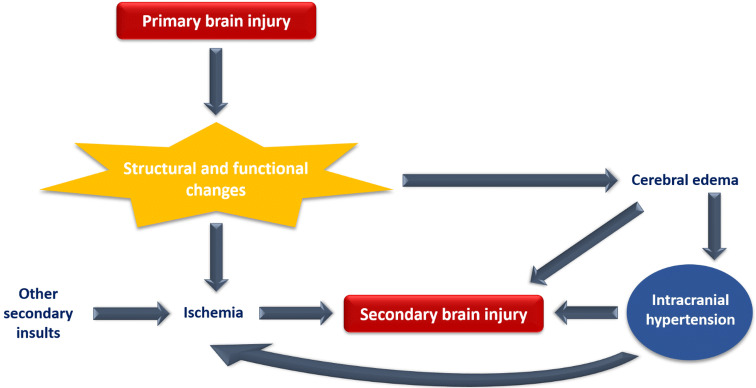
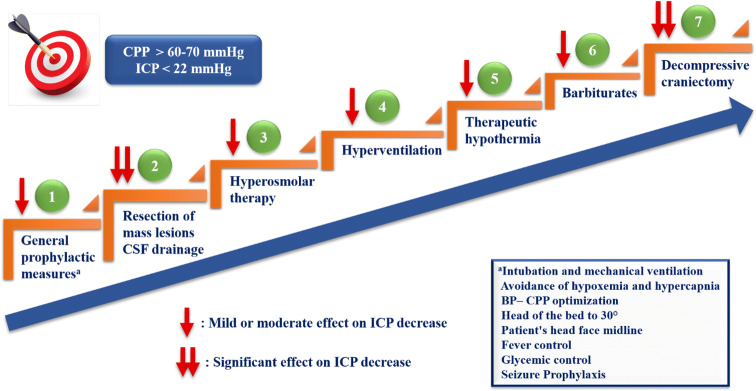
Intracranial hypertension (IH) is a clinical condition commonly encountered in the intensive care unit, which requires immediate treatment. The maintenance of normal intracranial pressure (ICP) and cerebral perfusion pressure in order to prevent secondary brain injury (SBI) is the central focus of management. SBI can be detected through clinical examination and invasive and non-invasive ICP monitoring. Progress in monitoring and understanding the pathophysiological mechanisms of IH allows the implementation of targeted interventions in order to improve the outcome of these patients. Initially, general prophylactic measures such as patient's head elevation, fever control, adequate analgesia and sedation depth should be applied immediately to all patients with suspected IH. Based on specific indications and conditions, surgical resection of mass lesions and cerebrospinal fluid drainage should be considered as an initial treatment for lowering ICP. Hyperosmolar therapy (mannitol or hypertonic saline) represents the cornerstone of medical treatment of acute IH while hyperventilation should be limited to emergency management of life-threatening raised ICP. Therapeutic hypothermia could have a possible benefit on outcome. To control elevated ICP refractory to maximum standard medical and surgical treatment, at first, high-dose barbiturate administration and then decompressive craniectomy as a last step are recommended with unclear and probable benefit on outcomes, respectively. The therapeutic strategy should be based on a staircase approach and be individualized for each patient. Since most therapeutic interventions have an uncertain effect on neurological outcome and mortality, future research should focus on both studying the long-term benefits of current strategies and developing new ones.
颅内高压(IH)是重症监护病房中常见的临床病症,需要立即进行治疗。维持正常颅内压(ICP)和脑灌注压以预防继发性脑损伤(SBI)是管理的核心重点。SBI 可以通过临床检查以及有创和无创 ICP 监测进行检测。监测和理解 IH 的病理生理机制方面的进展使我们能够实施针对性干预措施,从而改善这些患者的预后。最初,所有疑似 IH 的患者均应立即应用一般预防性措施,如抬高患者头部、控制发热、充分镇痛和镇静深度。基于具体的适应证和情况,应考虑手术切除肿块病变和脑脊液引流作为降低 ICP 的初始治疗方法。高渗治疗(甘露醇或高渗盐水)是急性 IH 医学治疗的基石,而过度通气应仅限于危及生命的 ICP 升高的紧急处理。治疗性低温可能对结局有一定益处。对于对最大标准的药物和手术治疗仍无法控制的 ICP 升高,建议首先使用大剂量巴比妥类药物治疗,然后作为最后一步进行减压性颅骨切除术,这两种方法对结局的益处分别不太明确和可能有益。治疗策略应基于阶梯式方法,并针对每个患者进行个体化。由于大多数治疗干预措施对神经功能预后和死亡率的影响不确定,因此未来的研究应侧重于研究当前策略的长期益处和开发新策略。