Seo Hyun Ju, Lee Na Rae, Son Soo Kyung, Kim Dae Keun, Rha Koon Ho, Lee Seon Heui
Department of Nursing, College of Medicine, Chosun University, Gwangju, Korea.
Department of Health Technology Assessment, National Evidence-based Healthcare Collaborating Agency, Seoul, Korea.
Yonsei Med J. 2016 Sep;57(5):1165-77. doi: 10.3349/ymj.2016.57.5.1165.
To systematically update evidence on the clinical efficacy and safety of robot-assisted radical prostatectomy (RARP) versus retropubic radical prostatectomy (RRP) in patients with prostate cancer.
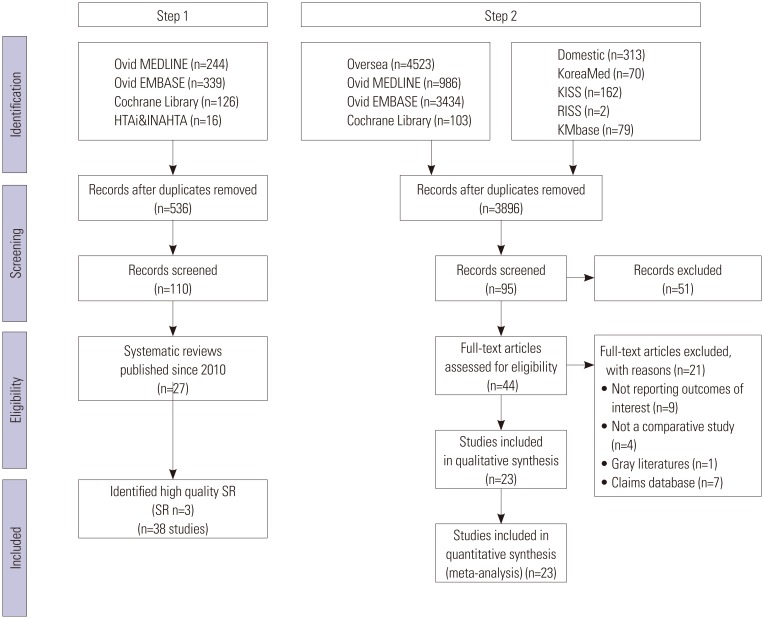
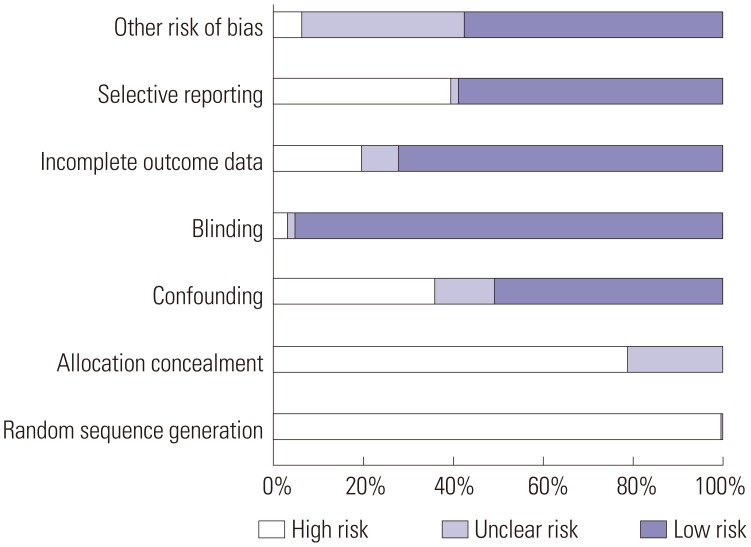
Electronic databases, including ovidMEDLINE, ovidEMBASE, the Cochrane Library, KoreaMed, KMbase, and others, were searched, collecting data from January 1980 to August 2013. The quality of selected systematic reviews was assessed using the revised assessment of multiple systematic reviews and the modified Cochrane Risk of Bias tool for non-randomized studies.
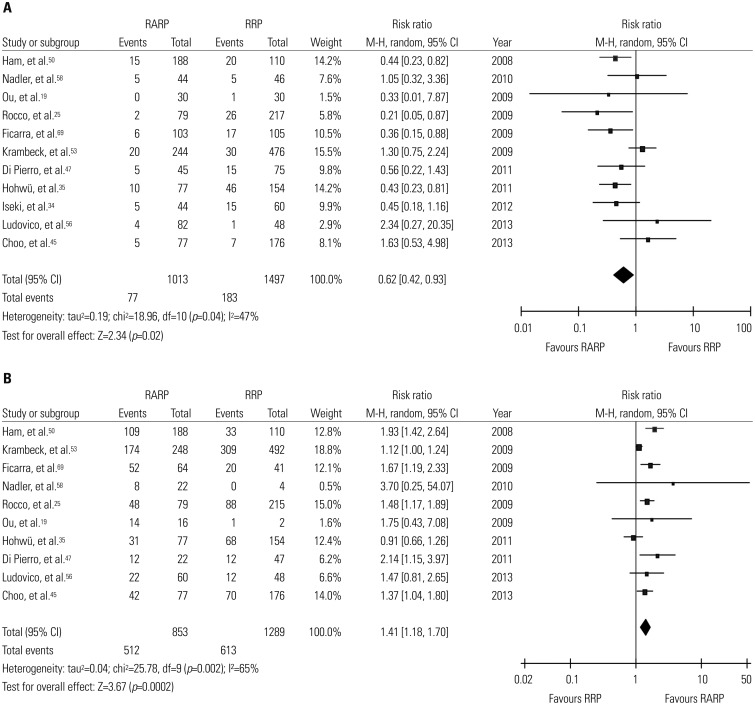
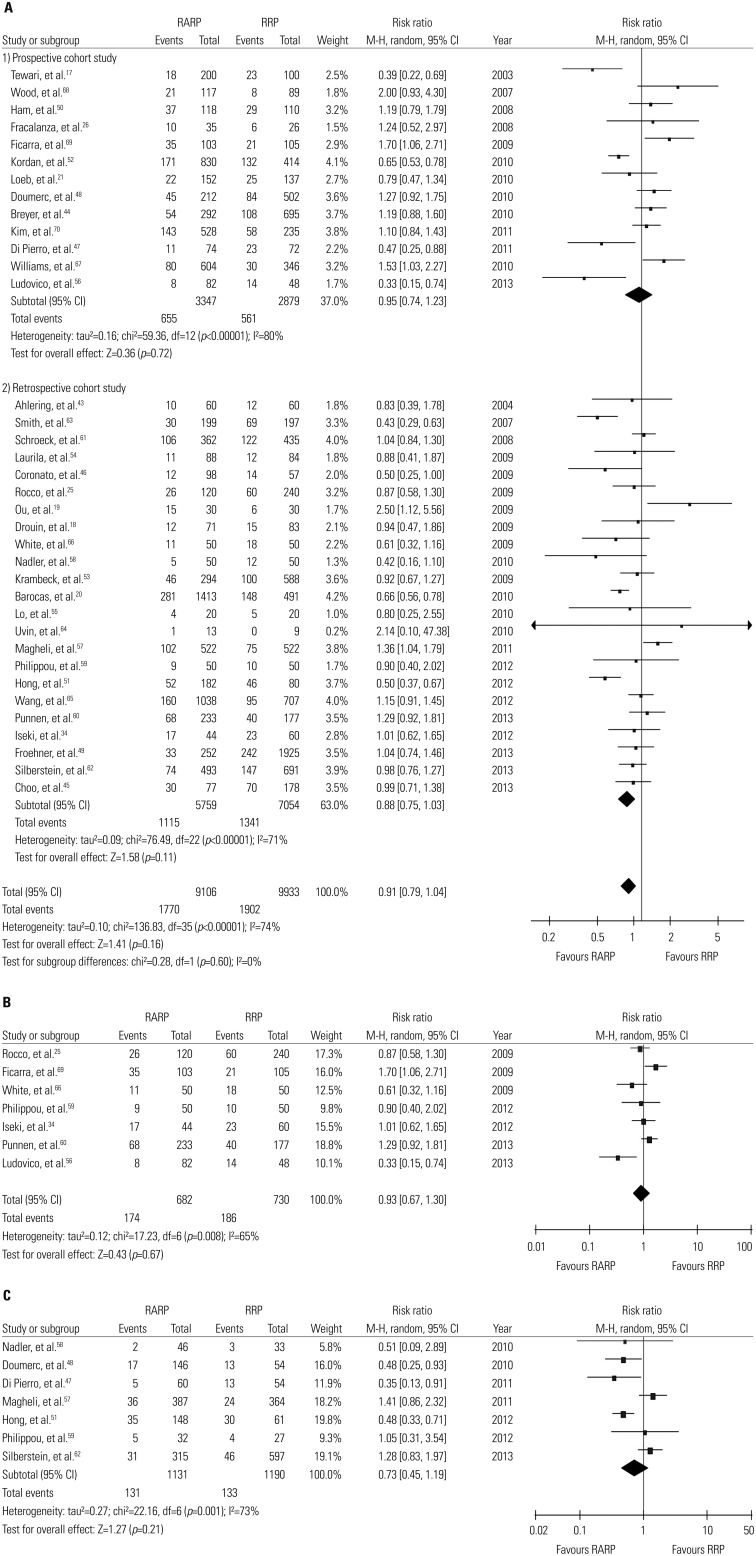
A total of 61 studies were included, including 38 from two previous systematic reviews rated as best available evidence and 23 additional studies that were more recent. There were no randomized controlled trials. Regarding safety, the risk of complications was lower for RARP than for RRP. Among functional outcomes, the risk of urinary incontinence was lower and potency rate was significantly higher for RARP than for RRP. Regarding oncologic outcomes, positive margin rates were comparable between groups, and although biochemical recurrence (BCR) rates were lower for RARP than for RRP, recurrence-free survival was similar after long-term follow up.
RARP might be favorable to RRP in regards to post-operative complications, peri-operative outcomes, and functional outcomes. Positive margin and BCR rates were comparable between the two procedures. As most of studies were of low quality, the results presented should be interpreted with caution, and further high quality studies controlling for selection, confounding, and selective reporting biases with longer-term follow-up are needed to determine the clinical efficacy and safety of RARP.
系统更新关于机器人辅助根治性前列腺切除术(RARP)与耻骨后根治性前列腺切除术(RRP)治疗前列腺癌患者的临床疗效和安全性的证据。
检索电子数据库,包括ovidMEDLINE、ovidEMBASE、Cochrane图书馆、KoreaMed、KMbase等,收集1980年1月至2013年8月的数据。使用修订后的多个系统评价评估和针对非随机研究的改良Cochrane偏倚风险工具评估所选系统评价的质量。
共纳入61项研究,包括之前两项系统评价中被评为最佳现有证据的38项研究以及另外23项更新的研究。没有随机对照试验。在安全性方面,RARP的并发症风险低于RRP。在功能结局方面,RARP的尿失禁风险较低,性功能恢复率显著高于RRP。在肿瘤学结局方面,两组的切缘阳性率相当,虽然RARP的生化复发(BCR)率低于RRP,但长期随访后的无复发生存率相似。
在术后并发症、围手术期结局和功能结局方面,RARP可能优于RRP。两种手术的切缘阳性率和BCR率相当。由于大多数研究质量较低,所呈现的结果应谨慎解释,需要进一步开展高质量研究,控制选择、混杂和选择性报告偏倚,并进行长期随访,以确定RARP的临床疗效和安全性。