Depiazzi Julie, Everard Mark L
Physiotherapy Dept, Princess Margaret Hospital, Subiaco, Australia.
Dept of Respiratory Medicine, Princess Margaret Hospital, Subiaco, Australia; University of Western Australia, Crawley, Australia.
Breathe (Sheff). 2016 Jun;12(2):120-9. doi: 10.1183/20734735.007216.
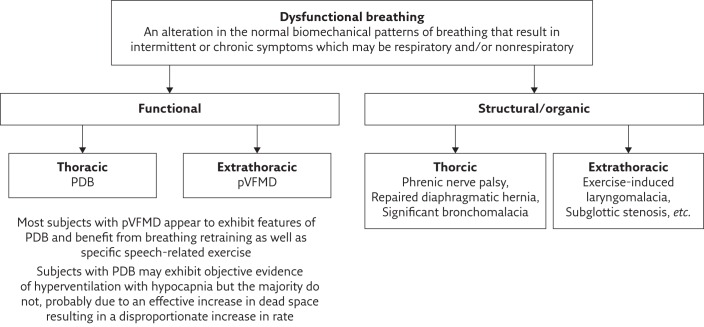
Excessive exercise-induced shortness of breath is a common complaint. For some, exercise-induced bronchoconstriction is the primary cause and for a small minority there may be an alternative organic pathology. However for many, the cause will be simply reaching their physiological limit or be due to a functional form of dysfunctional breathing, neither of which require drug therapy.The physiological limit category includes deconditioned individuals, such as those who have been through intensive care and require rehabilitation, as well as the unfit and the fit competitive athlete who has reached their limit with both of these latter groups requiring explanation and advice.Dysfunctional breathing is an umbrella term for an alteration in the normal biomechanical patterns of breathing that result in intermittent or chronic symptoms, which may be respiratory and/or nonrespiratory. This alteration may be due to structural causes or, much more commonly, be functional as exemplified by thoracic pattern disordered breathing (PDB) and extrathoracic paradoxical vocal fold motion disorder (pVFMD).Careful history and examination together with spirometry may identify those likely to have PDB and/or pVFMD. Where there is doubt about aetiology, cardiopulmonary exercise testing may be required to identify the deconditioned, unfit or fit individual reaching their physiological limit and PDB, while continuous laryngoscopy during exercise is increasingly becoming the benchmark for assessing extrathoracic causes.Accurate assessment and diagnosis can prevent excessive use of drug therapy and result in effective management of the cause of the individual's complaint through cost-effective approaches such as reassurance, advice, breathing retraining and vocal exercises. This review provides an overview of the spectrum of conditions that can present as exercise--induced breathlessness experienced by young subjects participating in sport and aims to promote understanding of the need for accurate assessment of an individual's symptoms. We will highlight the high incidence of nonasthmatic causes, which simply require reassurance or simple interventions from respiratory physiotherapists or speech pathologists.
运动过度导致的呼吸急促是一种常见的主诉。对一些人来说,运动诱发的支气管收缩是主要原因,而对少数人来说,可能存在其他器质性病变。然而,对许多人来说,原因仅仅是达到了他们的生理极限,或者是由于功能性呼吸功能障碍,这两种情况都不需要药物治疗。生理极限类别包括身体机能失调的个体,如那些经历过重症监护需要康复的人,以及身体不健康的人和达到极限的健康竞技运动员,后两类人都需要解释和建议。呼吸功能障碍是一个统称,指正常呼吸生物力学模式的改变,导致间歇性或慢性症状,这些症状可能是呼吸系统和/或非呼吸系统的。这种改变可能是由于结构原因,或者更常见的是功能性原因,如胸式呼吸模式紊乱(PDB)和胸外矛盾性声带运动障碍(pVFMD)。仔细的病史询问、体格检查以及肺功能测试可能会识别出那些可能患有PDB和/或pVFMD的人。如果对病因存在疑问,可能需要进行心肺运动测试,以识别身体机能失调、不健康或达到生理极限的个体以及PDB,而运动期间的连续喉镜检查越来越成为评估胸外病因的基准。准确的评估和诊断可以避免过度使用药物治疗,并通过成本效益高的方法,如安慰、建议、呼吸再训练和发声练习,有效管理个体主诉的病因。本综述概述了参与运动的年轻受试者可能出现的运动诱发呼吸困难的一系列情况,旨在促进对准确评估个体症状必要性的理解。我们将强调非哮喘病因的高发生率,这些病因只需要呼吸治疗师或言语病理学家的安慰或简单干预。