Bek S, Nielsen J V, Bojesen A B, Franke A, Bank S, Vogel U, Andersen V
Molecular and Diagnostic Research Unit, Hospital of Southern Jutland, Aabenraa, Denmark.
Research Unit for E-mental Health, Mental Health Services in the Region of Southern Odense, Odense, Denmark.
Aliment Pharmacol Ther. 2016 Sep;44(6):554-67. doi: 10.1111/apt.13736. Epub 2016 Jul 15.
Personalised medicine, including biomarkers for treatment selection, may provide new algorithms for more effective treatment of patients. Genetic variation may impact drug response and genetic markers could help selecting the best treatment strategy for the individual patient.
To identify polymorphisms and candidate genes from the literature that are associated with anti-tumour necrosis factor (TNF) treatment response in patients with inflammatory bowel diseases (IBD), Crohn's disease (CD) and ulcerative colitis.
We performed a PubMed literature search and retrieved studies reporting original data on association between polymorphisms and anti-TNF treatment response and conducted a meta-analysis.
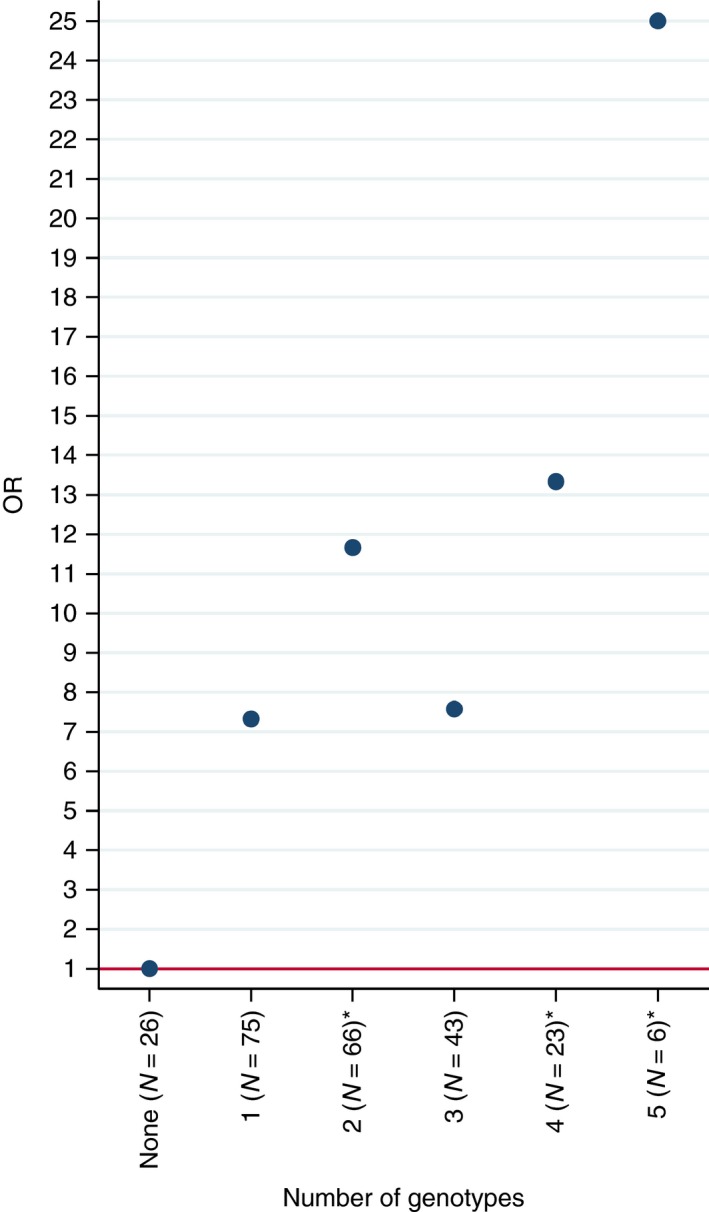
A functional polymorphism in FCGR3A was significantly associated with anti-TNF treatment response among CD patients using biological response criterion (decrease in C-reactive protein, levels). Meta-analyses showed that polymorphisms in TLR2 (rs3804099, OR (95% CI) = 2.17 (1.35-3.47)], rs11938228 [OR = 0.64 (0.43-0.96)], TLR4 (rs5030728) [OR = 3.18 (1.63-6.21)], TLR9 (rs352139) [OR = 0.43 (0.21-0.88)], TNFRSF1A (rs4149570) [OR = 2.06 (1.02-4.17)], IFNG (rs2430561) [OR = 1.66 (1.05-2.63)], IL6 (rs10499563) [OR = 1.65 (1.04-2.63)] and IL1B (rs4848306) [OR = 1.88 (1.05-3.35)] were significantly associated with response among IBD patients using clinical response criteria. A positive predictive value of 0.96 was achieved by combining five genetic markers in an explorative analysis.
There are no genetic markers currently available which are adequately predictive of anti-TNF response for use in the clinic. Genetic markers bear the advantage that they do not change over time. Therefore, hypothesis-free approaches, testing a large number of polymorphisms in large, well-characterised cohorts, are required in order to identify genetic profiles with larger effect sizes, which could be employed as biomarkers for treatment selection in clinical settings.
个性化医疗,包括用于治疗选择的生物标志物,可能为更有效地治疗患者提供新的算法。基因变异可能影响药物反应,基因标记有助于为个体患者选择最佳治疗策略。
从文献中识别与炎症性肠病(IBD)、克罗恩病(CD)和溃疡性结肠炎患者抗肿瘤坏死因子(TNF)治疗反应相关的多态性和候选基因。
我们进行了PubMed文献检索,检索报告多态性与抗TNF治疗反应之间关联的原始数据的研究,并进行了荟萃分析。
使用生物学反应标准(C反应蛋白水平降低)时,FCGR3A中的功能性多态性与CD患者的抗TNF治疗反应显著相关。荟萃分析表明,使用临床反应标准时,TLR2(rs3804099,OR(95%CI)=2.17(1.35 - 3.47))、rs11938228(OR = 0.64(0.43 - 0.96))、TLR4(rs5030728)(OR = 3.18(1.63 - 6.21))、TLR9(rs352139)(OR = 0.43(0.21 - 0.88))、TNFRSF1A(rs4149570)(OR = 2.06(1.02 - 4.17))、IFNG(rs2430561)(OR = 1.66(1.05 - 2.63))、IL6(rs10499563)(OR = 1.65(1.04 - 2.63))和IL1B(rs4848306)(OR = 1.88(1.05 - 3.35))中的多态性与IBD患者的反应显著相关。在一项探索性分析中,通过组合五个基因标记实现了0.96的阳性预测值。
目前尚无足够预测临床抗TNF反应的基因标记。基因标记具有不随时间变化的优势。因此,需要采用无假设方法,在大型、特征明确的队列中检测大量多态性,以识别效应大小更大的基因谱,可将其用作临床治疗选择的生物标志物。