Christensen Heidi Dahl, Sheta Hussam Mahmoud, Morillon Melanie Birger, Hansen Inger Marie Jensen
Department of Rheumatology, Odense University Hospital, Svendborg Hospital, Svendborg, Denmark.
Department of Medical Research, Odense University Hospital, Svendborg Hospital, Svendborg, Denmark.
Am J Case Rep. 2016 Jul 15;17:494-8. doi: 10.12659/ajcr.898542.
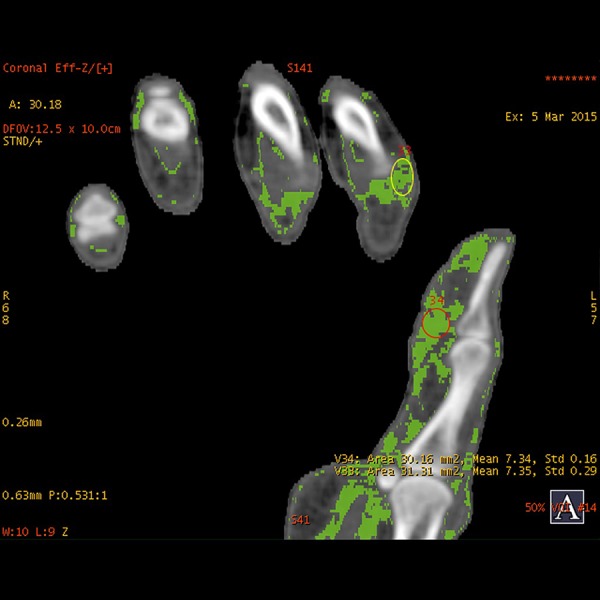
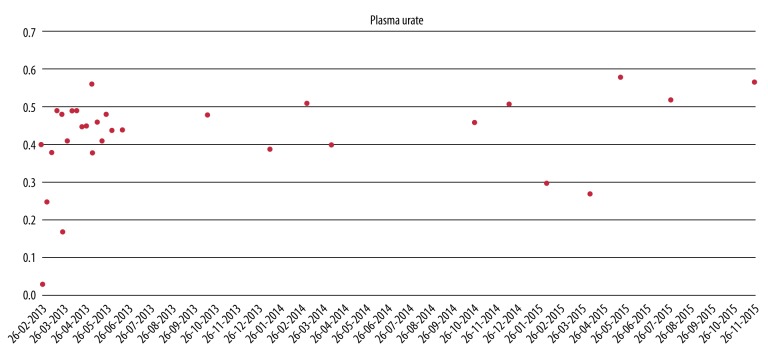
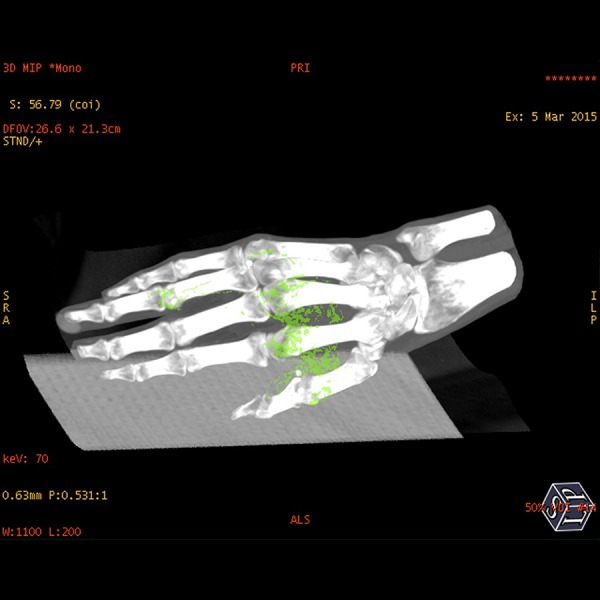
BACKGROUND Gout is characterized by deposition of uric acid crystals (monosodium urate) in tissues and fluids. This can cause acute inflammatory arthritis. The 2015 ACR/EULAR criteria for the diagnosis of gout include dual energy computed tomography (DECT)-demonstrated monosodium urate crystals as a new criterion. DECT is a spectral decomposition that permits recognition of different types of tissues based on their characteristic energy-dependent photon attenuation. A positive scan is defined as the presence of urate at articular or periarticular sites. CASE REPORT We describe a 51-year-old woman known to have anorexia nervosa. During our clinical examination, we detected plenty of tophi on both hands, but no swollen joints. The diagnosis of gout was made by visualizing crystals in a biopsy from a tophus. The first line of treatment was allopurinol, the second line was rasburicase, and the current treatment is febuxostat 80 mg/day, allopurinol 300 mg twice a day, and colchicine 0.5 mg twice a day. The patient has unchanged arthralgia and the size and number of tophi remain the same as before treatment in spite of active treatment for 3 years. Previously the patient had problems with adherence, but now she claims that she follows the proposed treatment. The last plasma urate (P-urate) was 0.57 mmol/L. Following two years of treatment, DECT of hands visualized monosodium urate crystal deposits in the tophi, as seen on the clinical photos, but also crystals in relation to the tendons and soft tissue. CONCLUSIONS DECT is an imaging modality useful to assess urate crystal deposits at diagnosis of gout and could be considered during treatment evaluation. Lack of adherence to treatment should be considered when P-urate values vary significantly and when DECT scans over years persistently visualize monosodium urate crystals.
痛风的特征是尿酸晶体(尿酸钠)在组织和体液中沉积。这可导致急性炎症性关节炎。2015年美国风湿病学会(ACR)/欧洲抗风湿病联盟(EULAR)痛风诊断标准将双能计算机断层扫描(DECT)显示的尿酸钠晶体作为一项新的标准。DECT是一种光谱分解技术,可根据不同组织的特征性能量依赖性光子衰减来识别不同类型的组织。阳性扫描定义为关节或关节周围部位存在尿酸盐。
我们描述了一名已知患有神经性厌食症的51岁女性。在临床检查过程中,我们在其双手发现了大量痛风石,但关节无肿胀。通过对痛风石活检中晶体的可视化检查确诊为痛风。一线治疗药物为别嘌醇,二线为重组尿酸氧化酶,目前的治疗方案是非布司他80mg/天、别嘌醇300mg每日两次以及秋水仙碱0.5mg每日两次。尽管积极治疗了3年,但患者的关节痛没有变化,痛风石的大小和数量仍与治疗前相同。该患者之前存在依从性问题,但现在她声称遵循了建议的治疗方案。末次血浆尿酸(P-尿酸)为0.57mmol/L。经过两年治疗,双手的DECT显示痛风石中有尿酸钠晶体沉积,如临床照片所示,同时在肌腱和软组织中也发现了晶体。
DECT是一种有助于评估痛风诊断时尿酸盐晶体沉积的成像方式,在治疗评估时可予以考虑。当P-尿酸值显著变化以及多年的DECT扫描持续显示尿酸钠晶体时,应考虑患者存在治疗依从性不佳的情况。