Jardim Denis Leonardo, Schwaederle Maria, Hong David S, Kurzrock Razelle
Department of Clinical Oncology, Hospital Sirio Libanes, Sao Paulo, Brazil.
Center for Personalized Cancer Therapy and Division of Hematology and Oncology, University of California, San Diego, CA, USA.
Oncotarget. 2016 Aug 16;7(33):53037-53046. doi: 10.18632/oncotarget.10588.
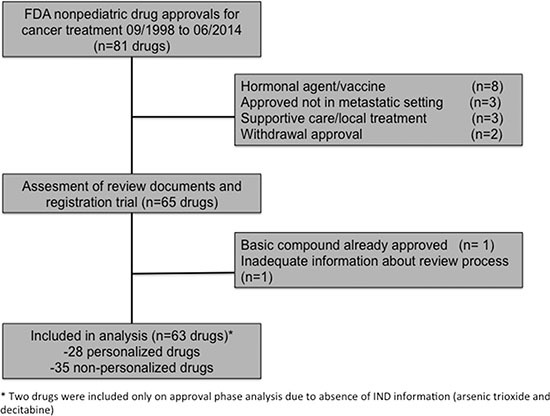
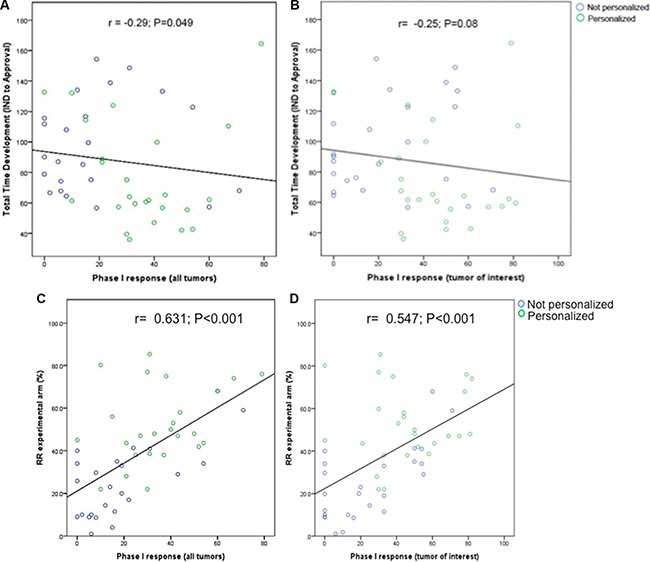
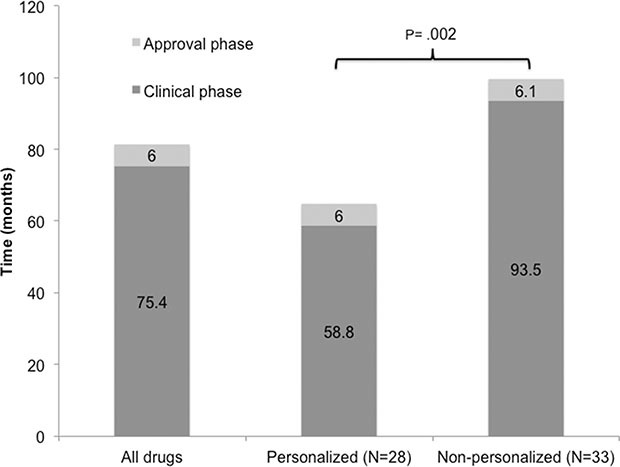
The effects of incorporating a biomarker-based (personalized or precision) selection strategy on drug development timelines for new oncology drugs merit investigation. Here we accessed documents from the Food and Drug Administration (FDA) database for anticancer agents approved between 09/1998 and 07/2014 to compare drugs developed with and without a personalized strategy. Sixty-three drugs were included (28 [44%] personalized and 35 [56%] non-personalized). No differences in access to FDA-expedited programs were observed between personalized and non-personalized drugs. A personalized approach for drug development was associated with faster clinical development (Investigational New Drug [IND] to New Drug Application [NDA] submission; median = 58.8 months [95% CI 53.8-81.8] vs. 93.5 months [95% CI 73.9-112.9], P =.001), but a similar approval time (NDA submission to approval; median=6.0 months [95% CI 5.5-8.4] vs. 6.1 months [95% CI 5.9-8.3], P = .756) compared to a non-personalized strategy. In the multivariate model, class of drug stratified by personalized status (targeted personalized vs. targeted non-personalized vs. cytotoxic) was the only independent factor associated with faster total time of clinical drug development (clinical plus approval phase, median = 64.6 vs 87.1 vs. 112.7 months [cytotoxic], P = .038). Response rates (RR) in early trials were positively correlated with RR in registration trials (r = 0.63, P = <.001), and inversely associated with total time of drug development (r = -0.29, P = .049). In conclusion, targeted agents were developed faster than cytotoxic agents. Shorter times to approval were associated, in multivariate analysis, with a biomarker-based clinical development strategy.
采用基于生物标志物的(个性化或精准)选择策略对新型肿瘤药物研发时间表的影响值得研究。在此,我们查阅了美国食品药品监督管理局(FDA)数据库中1998年9月至2014年7月间获批的抗癌药物文件,以比较采用和未采用个性化策略研发的药物。共纳入63种药物(28种[44%]为个性化药物,35种[56%]为非个性化药物)。个性化药物和非个性化药物在进入FDA加速项目方面未观察到差异。药物研发的个性化方法与更快的临床研发相关(从研究性新药[IND]申请到新药申请[NDA]提交;中位数=58.8个月[95%CI 53.8 - 81.8]对比93.5个月[95%CI 73.9 - 112.9],P =.001),但与非个性化策略相比,批准时间相似(从NDA提交到批准;中位数=6.0个月[95%CI 5.5 - 8.4]对比6.1个月[95%CI 5.9 - 8.3],P =.756)。在多变量模型中,按个性化状态分层的药物类别(靶向个性化药物对比靶向非个性化药物对比细胞毒性药物)是与临床药物研发总时间更快相关的唯一独立因素(临床加批准阶段,中位数分别为64.6、87.1和112.7个月[细胞毒性药物],P =.038)。早期试验中的缓解率(RR)与注册试验中的RR呈正相关(r = 0.63,P =<.001),且与药物研发总时间呈负相关(r = -0.29,P =.049)。总之,靶向药物的研发速度比细胞毒性药物更快。在多变量分析中,较短的批准时间与基于生物标志物的临床研发策略相关。