Wang Hao, Umejiego Johnbosco, Robinson Richard D, Schrader Chet D, Leuck JoAnna, Barra Michael, Buca Stefan, Shedd Andrew, Bui Andrew, Zenarosa Nestor R
Department of Emergency Medicine, Integrative Emergency Services, John Peter Smith Health Network, 1500 S. Main St., Fort Worth, TX 76104, USA.
J Clin Med Res. 2016 Aug;8(8):591-7. doi: 10.14740/jocmr2598w. Epub 2016 Jul 1.
There is no existing adequate blood transfusion needs determination tool that Emergency Medical Services (EMS) personnel can use for prehospital blood transfusion initiation. In this study, a simple and pragmatic prehospital blood transfusion needs scoring system was derived and validated.
Local trauma registry data were reviewed retrospectively from 2004 through 2013. Patients were randomly assigned to derivation and validation cohorts. Multivariate logistic regression was used to identify the independent approachable risks associated with early blood transfusion needs in the derivation cohort in which a scoring system was derived. Sensitivity, specificity, and area under the receiver operational characteristic (AUC) were calculated and compared using both the derivation and validation data.
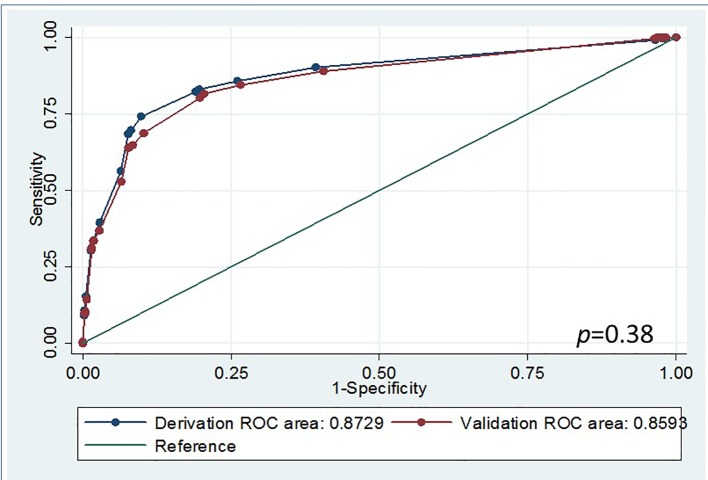
A total of 24,303 patients were included with 12,151 patients in the derivation and 12,152 patients in the validation cohorts. Age, penetrating injury, heart rate, systolic blood pressure, and Glasgow coma scale (GCS) were risks predictive of early blood transfusion needs. An early blood transfusion needs score was derived. A score > 5 indicated risk of early blood transfusion need with a sensitivity of 83% and a specificity of 80%. A sensitivity of 82% and a specificity of 80% were also found in the validation study and their AUC showed no statistically significant difference (AUC of the derivation = 0.87 versus AUC of the validation = 0.86, P > 0.05).
An early blood transfusion scoring system was derived and internally validated to predict severe trauma patients requiring blood transfusion during prehospital or initial emergency department resuscitation.
目前尚无足够的输血需求判定工具供紧急医疗服务(EMS)人员在院前启动输血时使用。在本研究中,我们推导并验证了一种简单实用的院前输血需求评分系统。
回顾性分析2004年至2013年当地创伤登记数据。患者被随机分配到推导队列和验证队列。在推导队列中使用多因素逻辑回归来识别与早期输血需求相关的独立可及风险,并推导评分系统。使用推导数据和验证数据计算并比较敏感性、特异性和受试者操作特征曲线下面积(AUC)。
共纳入24303例患者,其中推导队列12151例,验证队列12152例。年龄、穿透伤、心率、收缩压和格拉斯哥昏迷量表(GCS)是早期输血需求的预测风险因素。由此得出早期输血需求评分。评分>5表明有早期输血需求风险,敏感性为83%,特异性为80%。在验证研究中也发现敏感性为82%,特异性为80%,且其AUC无统计学显著差异(推导队列的AUC = 0.87,验证队列的AUC = 0.86,P>0.05)。
推导并内部验证了一种早期输血评分系统,以预测在院前或急诊科初始复苏期间需要输血的严重创伤患者。