Strandberg Eva Lena, Brorsson Annika, André Malin, Gröndal Hedvig, Mölstad Sigvard, Hedin Katarina
Department of Clinical Sciences, Malmö, Family Medicine, Lund University, Malmö, Sweden.
Blekinge Centre of Competence, Blekinge County Council, Karlskrona, Sweden.
BMC Fam Pract. 2016 Jul 18;17:78. doi: 10.1186/s12875-016-0494-z.
Prescribing of antibiotics for common infections varies widely, and there is no medical explanation. Systematic reviews have highlighted factors that may influence antibiotic prescribing and that this is a complex process. It is unclear how factors interact and how the primary care organization affects diagnostic procedures and antibiotic prescribing. Therefore, we sought to explore and understand interactions between factors influencing antibiotic prescribing for respiratory tract infections in primary care.
Our mixed methods design was guided by the Triangulation Design Model according to Creswell. Quantitative and qualitative data were collected in parallel. Quantitative data were collected by prescription statistics, questionnaires to patients, and general practitioners' audit registrations. Qualitative data were collected through observations and semi-structured interviews.
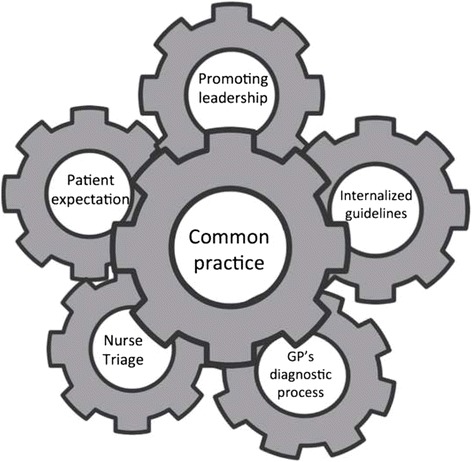
From the analysis of the data from the different sources an overall theme emerged: A common practice in the primary health care centre is crucial for low antibiotic prescribing in line with guidelines. Several factors contribute to a common practice, such as promoting management and leadership, internalized guidelines including inter-professional discussions, the general practitioner's diagnostic process, nurse triage, and patient expectation. These factors were closely related and influenced each other. The results showed that knowledge must be internalized and guidelines need to be normative for the group as well as for every individual.
Low prescribing is associated with adapted and transformed guidelines within all staff, not only general practitioners. Nurses' triage and self-care advice played an important role. Encouragement from the management level stimulated inter-professional discussions about antibiotic prescribing. Informal opinion moulders talking about antibiotic prescribing was supported by the managers. Finally, continuous professional development activities were encouraged for up-to-date knowledge.
常见感染的抗生素处方差异很大,且缺乏医学解释。系统评价强调了可能影响抗生素处方的因素,且这是一个复杂的过程。目前尚不清楚这些因素如何相互作用,以及基层医疗组织如何影响诊断程序和抗生素处方。因此,我们试图探索并理解基层医疗中影响呼吸道感染抗生素处方的因素之间的相互作用。
我们的混合方法设计以克雷斯韦尔的三角设计模型为指导。定量和定性数据并行收集。定量数据通过处方统计、患者问卷和全科医生审核登记收集。定性数据通过观察和半结构式访谈收集。
通过对不同来源数据的分析,出现了一个总体主题:基层医疗中心的一种常见做法对于按照指南减少抗生素处方至关重要。有几个因素促成了这种常见做法,比如促进管理和领导力、内化指南(包括跨专业讨论)、全科医生的诊断过程、护士分诊和患者期望。这些因素密切相关且相互影响。结果表明,知识必须被内化,指南对于团队以及每个个体都需要具有规范性。
低处方率与所有工作人员(不仅是全科医生)采用并转变后的指南相关。护士分诊和自我护理建议发挥了重要作用。管理层的鼓励促进了关于抗生素处方的跨专业讨论。管理者支持非正式意见领袖谈论抗生素处方。最后,鼓励开展持续专业发展活动以获取最新知识。