Stevens Kathryn K, Denby Laura, Patel Rajan K, Mark Patrick B, Kettlewell Sarah, Smith Godfrey L, Clancy Marc J, Delles Christian, Jardine Alan G
BHF Cardiovascular Research Centre, Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, UK.
The Renal Transplant Unit, Western Infirmary, (Now based at The Queen Elizabeth University Hospital) Glasgow, UK.
Nephrol Dial Transplant. 2017 Oct 1;32(10):1617-1627. doi: 10.1093/ndt/gfw252.
Hyperphosphataemia is an independent risk factor for accelerated cardiovascular disease in chronic kidney disease (CKD), although the mechanism for this is poorly understood. We investigated the effects of sustained exposure to a high-phosphate environment on endothelial function in cellular and preclinical models, as well as in human subjects.
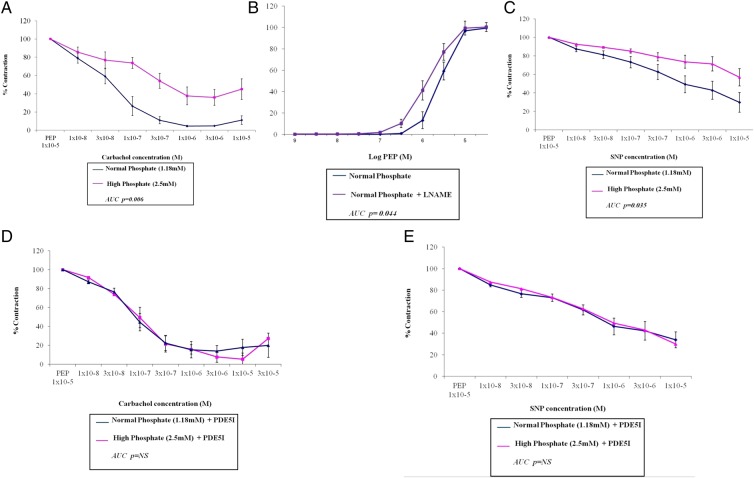
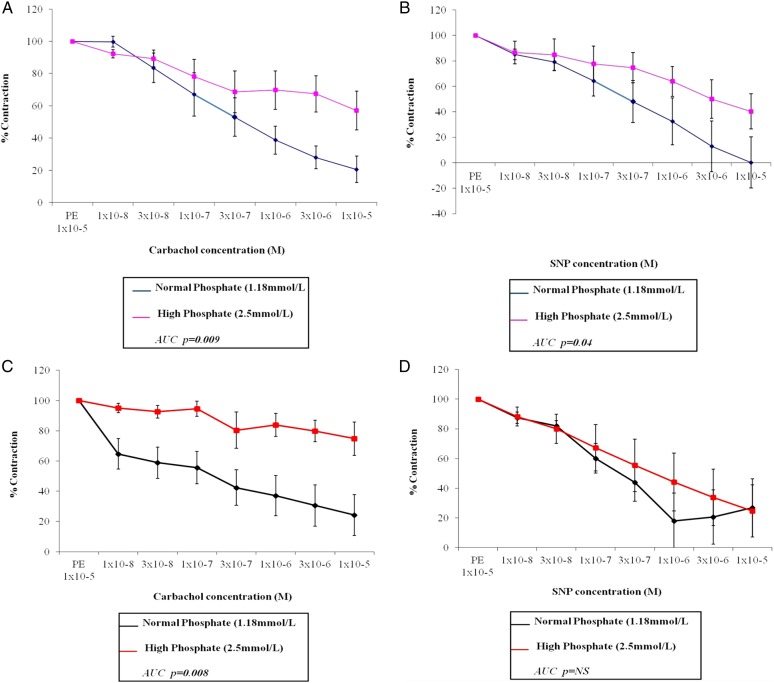
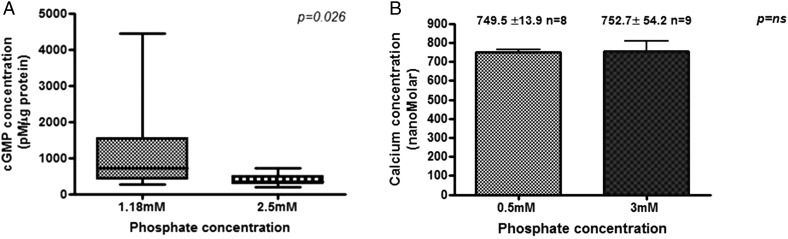
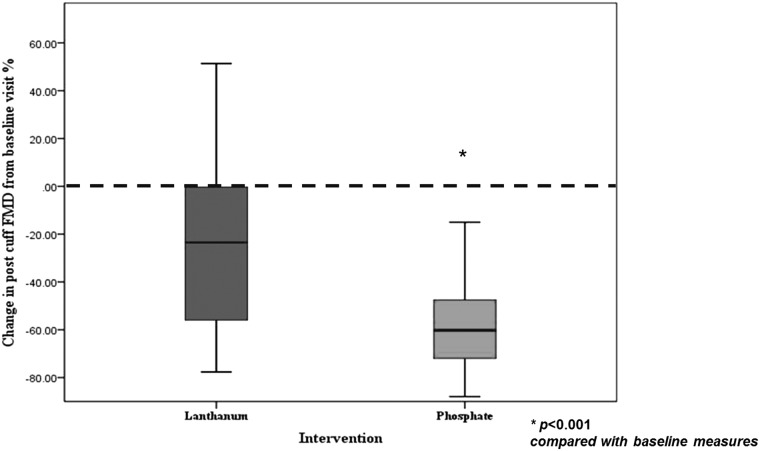
Resistance vessels from rats and humans (± CKD) were incubated in a normal (1.18 mM) or high (2.5 mM) phosphate concentration solution and cells were cultured in normal- (0.5 mM) or high-phosphate (3 mM) concentration media. A single-blind crossover study was performed in healthy volunteers, receiving phosphate supplements or a phosphate binder (lanthanum), and endothelial function measured was by flow-mediated dilatation.
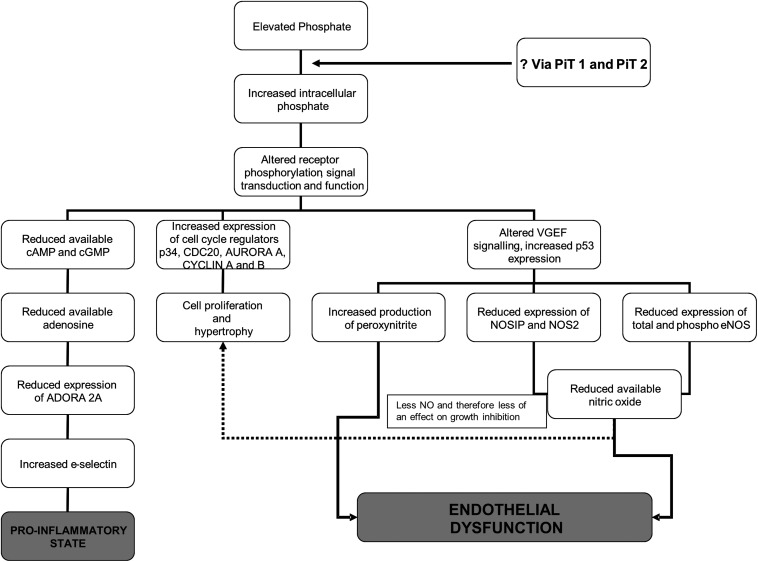
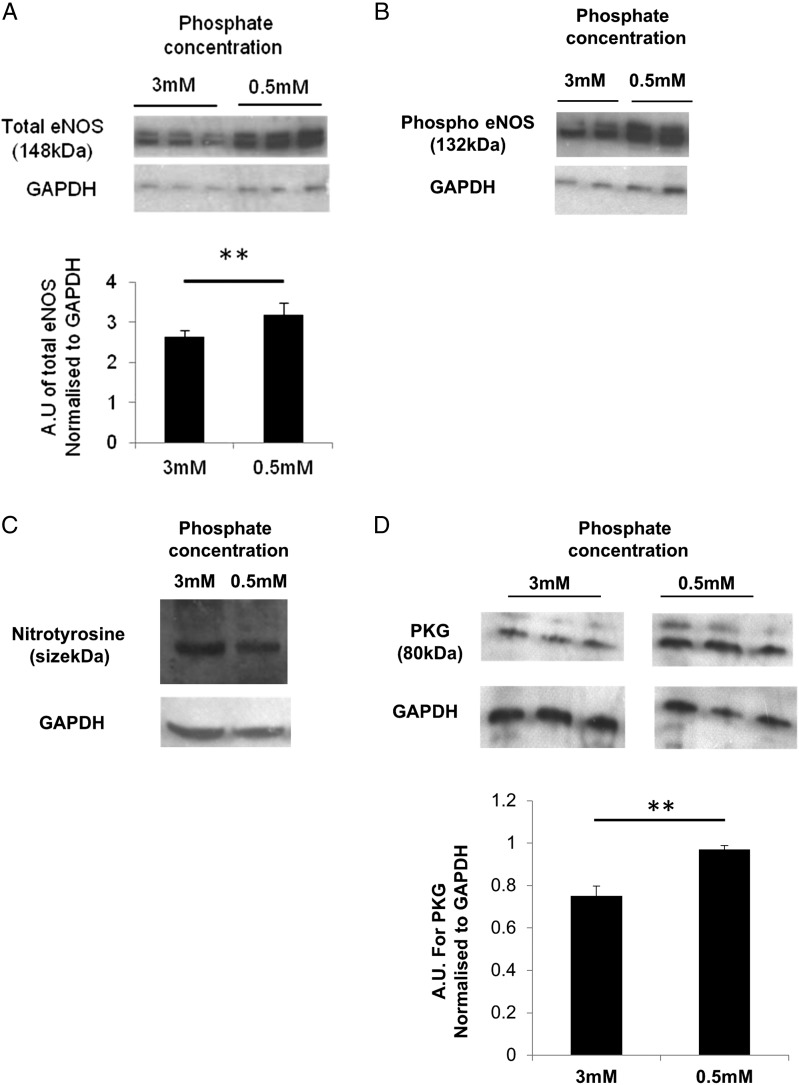
Endothelium-dependent vasodilatation was impaired when resistance vessels were exposed to high phosphate; this could be reversed in the presence of a phosphodiesterase-5-inhibitor. Vessels from patients with CKD relaxed normally when incubated in normal-phosphate conditions, suggesting that the detrimental effects of phosphate may be reversible. Exposure to high-phosphate disrupted the whole nitric oxide pathway with reduced nitric oxide and cyclic guanosine monophosphate production and total and phospho endothelial nitric oxide synthase expression. In humans, endothelial function was reduced by chronic phosphate loading independent of serum phosphate, but was associated with higher urinary phosphate excretion and serum fibroblast growth factor 23.
These directly detrimental effects of phosphate, independent of other factors in the uraemic environment, may explain the increased cardiovascular risk associated with phosphate in CKD.
高磷血症是慢性肾脏病(CKD)患者心血管疾病加速进展的独立危险因素,但其机制尚不清楚。我们在细胞模型、临床前模型以及人类受试者中研究了持续暴露于高磷环境对内皮功能的影响。
将大鼠和人类(±CKD)的阻力血管分别置于正常(1.18 mM)或高磷(2.5 mM)浓度的溶液中孵育,并将细胞培养于正常磷(0.5 mM)或高磷(3 mM)浓度的培养基中。对健康志愿者进行单盲交叉研究,给予磷补充剂或磷结合剂(镧),通过血流介导的血管舒张来测量内皮功能。
当阻力血管暴露于高磷环境时,内皮依赖性血管舒张功能受损;在磷酸二酯酶-5抑制剂存在的情况下,这种情况可以得到逆转。在正常磷条件下孵育时,CKD患者的血管舒张正常,这表明磷的有害作用可能是可逆的。暴露于高磷环境会破坏整个一氧化氮途径,导致一氧化氮和环磷酸鸟苷生成减少,以及总内皮型一氧化氮合酶和磷酸化内皮型一氧化氮合酶表达降低。在人类中,慢性磷负荷会降低内皮功能,这与血清磷无关,但与更高的尿磷排泄和血清成纤维细胞生长因子23水平有关。
磷的这些直接有害作用独立于尿毒症环境中的其他因素,这可能解释了CKD患者中与磷相关的心血管风险增加的原因。