Dartmouth College, Hanover, NH, United States.
JMIR Ment Health. 2016 Jul 27;3(3):e34. doi: 10.2196/mental.6348.
mHealth interventions that use mobile phones as instruments for illness management are gaining popularity. Research examining mobile phone‒based mHealth programs for people with psychosis has shown that these approaches are feasible, acceptable, and clinically promising. However, most mHealth initiatives involving people with schizophrenia have spanned periods ranging from a few days to several weeks and have typically involved participants who were clinically stable.
Our aim was to evaluate the viability of extended mHealth interventions for people with schizophrenia-spectrum disorders following hospital discharge. Specifically, we set out to examine the following: (1) Can individuals be engaged with a mobile phone intervention program during this high-risk period?, (2) Are age, gender, racial background, or hospitalization history associated with their engagement or persistence in using a mobile phone intervention over time?, and (3) Does engagement differ by characteristics of the mHealth intervention itself (ie, pre-programmed vs on-demand functions)?
We examined mHealth intervention use and demographic and clinical predictors of engagement in 342 individuals with schizophrenia-spectrum disorders who were given the FOCUS mobile phone intervention as part of a technology-assisted relapse prevention program during the 6-month high-risk period following hospitalization.
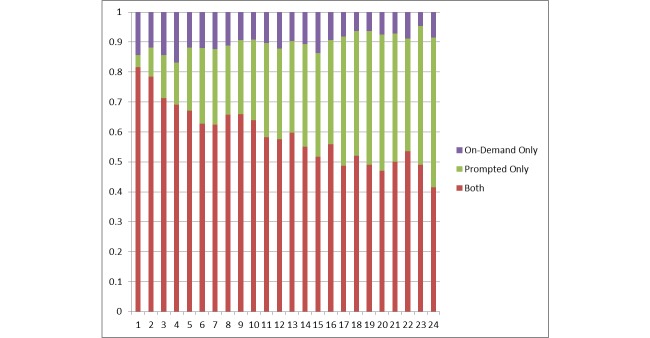
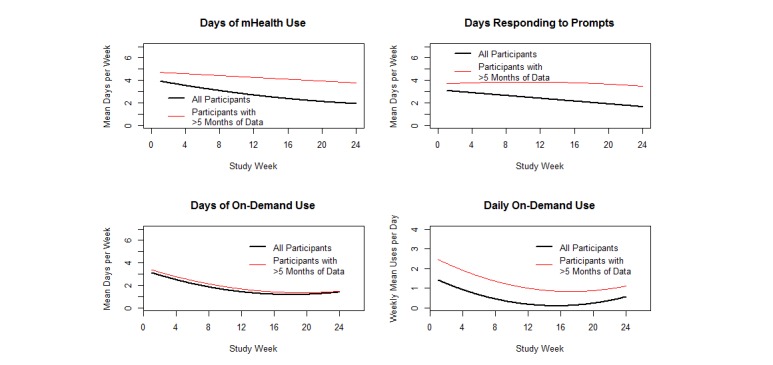
On average, participants engaged with FOCUS for 82% of the weeks they had the mobile phone. People who used FOCUS more often continued using it over longer periods: 44% used the intervention over 5-6 months, on average 4.3 days a week. Gender, race, age, and number of past psychiatric hospitalizations were associated with engagement. Females used FOCUS on average 0.4 more days a week than males. White participants engaged on average 0.7 days more a week than African-Americans and responded to prompts on 0.7 days more a week than Hispanic participants. Younger participants (age 18-29) had 0.4 fewer days of on-demand use a week than individuals who were 30-45 years old and 0.5 fewer days a week than older participants (age 46-60). Participants with fewer past hospitalizations (1-6) engaged on average 0.2 more days a week than those with seven or more. mHealth program functions were associated with engagement. Participants responded to prompts more often than they self-initiated on-demand tools, but both FOCUS functions were used regularly. Both types of intervention use declined over time (on-demand use had a steeper decline). Although mHealth use declined, the majority of individuals used both on-demand and system-prompted functions regularly throughout their participation. Therefore, neither function is extraneous.
The findings demonstrated that individuals with schizophrenia-spectrum disorders can actively engage with a clinically supported mobile phone intervention for up to 6 months following hospital discharge. mHealth may be useful in reaching a clinical population that is typically difficult to engage during high-risk periods.
使用手机进行疾病管理的移动医疗干预措施越来越受欢迎。研究表明,针对精神病患者的基于手机的移动医疗程序具有可行性、可接受性和临床前景。然而,大多数涉及精神分裂症患者的移动医疗计划的持续时间从几天到几周不等,并且通常涉及临床稳定的参与者。
我们旨在评估针对精神分裂症谱系障碍患者出院后的长期移动医疗干预措施的可行性。具体而言,我们旨在研究以下问题:(1)个体是否能够在这个高风险时期参与手机干预计划?(2)年龄、性别、种族背景或住院史是否与他们在一段时间内持续使用手机干预有关?(3)干预的参与程度是否因移动医疗干预本身的特点(即预编程功能与按需功能)而有所不同?
我们研究了 342 名精神分裂症谱系障碍患者的移动医疗干预使用情况以及参与度的人口统计学和临床预测因素,这些患者在出院后 6 个月的高风险期间被给予 FOCUS 手机干预,作为一种技术辅助的复发预防计划的一部分。
平均而言,参与者在使用手机的周数中,有 82%的时间参与了 FOCUS。更频繁使用 FOCUS 的人会持续使用更长时间:44%的人平均每周使用该干预措施 4.3 天。性别、种族、年龄和过去精神病住院次数与参与度相关。女性每周平均比男性多使用 FOCUS 0.4 天。白人参与者每周平均比非裔美国人多参与 0.7 天,比西班牙裔参与者每周多响应提示 0.7 天。年轻参与者(18-29 岁)每周的按需使用天数比 30-45 岁的参与者少 0.4 天,比 46-60 岁的参与者少 0.5 天。过去住院次数较少(1-6 次)的参与者每周平均比住院 7 次或以上的参与者多参与 0.2 天。移动医疗计划的功能与参与度相关。参与者比自我发起按需工具更频繁地响应提示,但两者都经常使用 FOCUS 功能。两种干预措施的使用都随时间减少(按需使用的下降更为陡峭)。尽管移动医疗的使用有所下降,但大多数参与者在整个参与过程中都定期使用按需和系统提示功能。因此,两种功能都不是多余的。
研究结果表明,精神分裂症谱系障碍患者可以在出院后长达 6 个月的时间内积极参与临床支持的手机干预措施。移动医疗可能对在高风险期间难以参与的临床人群有用。