Levison Julie H, Regan Susan, Khan Iman, Freedberg Kenneth A
a Division of General Internal Medicine , Massachusetts General Hospital , Boston , MA , USA.
b Harvard Medical School , Boston , MA , USA.
AIDS Care. 2017 Feb;29(2):244-251. doi: 10.1080/09540121.2016.1210077. Epub 2016 Jul 28.
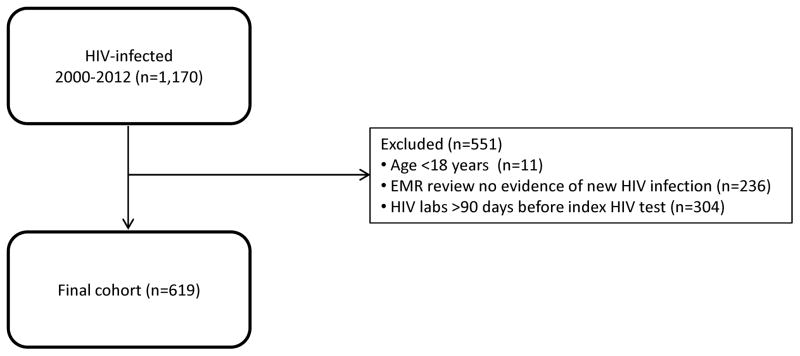
We sought to determine the linkage to and retention in HIV care after HIV diagnosis in foreign-born compared with US-born individuals. From a clinical data registry, we identified 619 patients aged ≥18 years with a new HIV diagnosis between 2000 and 2012. Timely linkage to care was the proportion of patients with an ICD-9 code for HIV infection (V08 or 042) associated with a primary care or infectious disease physician within 90 days of the index positive HIV test. Retention in HIV care was the presence of an HIV primary care visit in each 6-month period of the 24-month measurement period from the index HIV test. We used Cox regression analysis with adjustment for hypothesized confounders (age, gender, race/ethnicity, substance abuse, year, and location of HIV diagnosis). Foreign-born individuals comprised 36% (225/619) of the cohort. Index CD4 count was 225/µl (IQR 67-439/µl) in foreign-born compared with 328/µl (IQR 121-527/µl) in US-born individuals (p < .001). The proportion linked to care was 87% (196/225) in foreign-born compared with 77% (302/394) in US-born individuals (p = .002). The adjusted hazard ratio of linkage to HIV care in foreign-born compared with US-born individuals was 1.28 (95% confidence interval [CI], 1.05-1.56). Once linked, there was no difference in retention in care or virologic suppression at 24 months. These results show that despite late presentation to HIV care, foreign-born persons can subsequently engage in HIV care as well as US-born persons. Interventions that promote HIV screening in foreign-born persons are a promising way to improve outcomes in these populations.
我们试图确定与美国出生的个体相比,外国出生的个体在HIV诊断后与HIV治疗的关联及治疗的持续性。从一个临床数据登记处,我们识别出619名年龄≥18岁、在2000年至2012年间新诊断为HIV的患者。及时与治疗关联是指在首次HIV检测呈阳性后的90天内,具有HIV感染ICD-9编码(V08或042)且与初级保健医生或传染病医生相关联的患者比例。HIV治疗的持续性是指从首次HIV检测开始的24个月测量期内,每6个月有一次HIV初级保健就诊。我们使用Cox回归分析,并对假设的混杂因素(年龄、性别、种族/族裔、药物滥用、年份和HIV诊断地点)进行了调整。外国出生的个体占队列的36%(225/619)。外国出生个体的首次CD4细胞计数为225/µl(四分位间距67 - 439/µl),而美国出生个体为328/µl(四分位间距121 - 527/µl)(p < 0.001)。外国出生个体中与治疗关联的比例为87%(196/225),而美国出生个体为77%(302/394)(p = 0.002)。与美国出生个体相比,外国出生个体与HIV治疗关联的调整后风险比为1.28(95%置信区间[CI],1.05 - 1.56)。一旦建立关联,在24个月时的治疗持续性或病毒学抑制方面没有差异。这些结果表明,尽管外国出生的人较晚接受HIV治疗,但随后他们能像美国出生的人一样参与HIV治疗。促进外国出生人群进行HIV筛查的干预措施是改善这些人群治疗效果的一种有前景的方法。