Remien Robert H, Bauman Laurie J, Mantell Joanne E, Tsoi Benjamin, Lopez-Rios Javier, Chhabra Rosy, DiCarlo Abby, Watnick Dana, Rivera Angelic, Teitelman Nehama, Cutler Blayne, Warne Patricia
*HIV Center for Clinical and Behavioral Studies, NY State Psychiatric Institute and Columbia University, New York, NY; †Einstein-Montefiore Center for AIDS Research, Albert Einstein College of Medicine, New York, NY; ‡New York City Department of Health and Mental Hygiene, New York, NY; and §Public Health Foundation Enterprises, La Puente, CA.
J Acquir Immune Defic Syndr. 2015 May 1;69 Suppl 1(0 1):S16-24. doi: 10.1097/QAI.0000000000000577.
Engagement in HIV care helps to maximize viral suppression, which in turn, reduces morbidity and mortality and prevents further HIV transmission. With more HIV cases than any other US city, New York City reported in 2012 that only 41% of all persons estimated to be living with HIV (PLWH) had a suppressed viral load, whereas nearly three-quarters of those in clinical care achieved viral suppression. Thus, retaining PLWH in HIV care addresses this central goal of both the US National HIV/AIDS Strategy and Governor Cuomo's plan to end the AIDS epidemic in New York State.
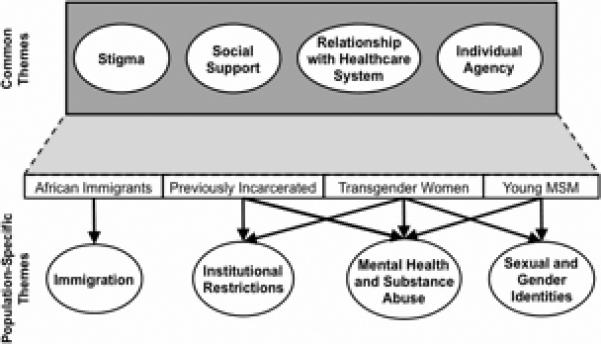
We conducted 80 in-depth qualitative interviews with PLWH in 4 New York City populations that were identified as being inconsistently engaged in HIV medical care: African immigrants, previously incarcerated adults, transgender women, and young men who have sex with men.
Barriers to and facilitators of HIV care engagement fell into 3 domains: (1) system factors (eg, patient-provider relationship, social service agencies, transitions between penal system and community), (2) social factors (eg, family and other social support; stigma related to HIV, substance use, sexual orientation, gender identity, and incarceration), and (3) individual factors (eg, mental illness, substance use, resilience). Similarities and differences in these themes across the 4 populations as well as research and public health implications were identified.
Engagement in care is maximized when the social challenges confronted by vulnerable groups are addressed, patient-provider communication is strong, and coordinated services are available, including housing, mental health and substance use treatment, and peer navigation.
接受艾滋病病毒治疗有助于最大限度地实现病毒抑制,进而降低发病率和死亡率,并防止艾滋病病毒的进一步传播。纽约市的艾滋病病例比美国其他任何城市都多,该市在2012年报告称,估计所有感染艾滋病病毒的人(PLWH)中只有41%的人病毒载量得到抑制,而在接受临床治疗的人中,近四分之三实现了病毒抑制。因此,让艾滋病病毒感染者持续接受治疗是美国国家艾滋病病毒/艾滋病战略以及纽约州州长安德鲁·科莫终结艾滋病流行计划的核心目标。
我们对纽约市4类被确定为未持续接受艾滋病病毒医疗护理的人群中的艾滋病病毒感染者进行了80次深入的定性访谈,这4类人群分别是非洲移民、曾被监禁的成年人、变性女性以及与男性发生性关系的年轻男性。
参与艾滋病病毒治疗的障碍和促进因素分为3个领域:(1)系统因素(如医患关系、社会服务机构、刑罚系统与社区之间的过渡),(2)社会因素(如家庭和其他社会支持;与艾滋病病毒、药物使用、性取向、性别认同和监禁相关的耻辱感),以及(3)个人因素(如精神疾病、药物使用、适应能力)。确定了这4类人群在这些主题上的异同以及研究和公共卫生方面的影响。
当弱势群体面临的社会挑战得到解决、医患沟通良好且有包括住房、心理健康和药物使用治疗以及同伴引导在内的协调服务时,治疗参与度将达到最大化。