Hiradfar Mehran, Gharavifard Mohammad, Shojaeian Reza, Joodi Marjan, Nazarzadeh Reza, Sabzevari Alireza, Yal Nazila, Eslami Reza, Mohammadipour Ahmad, Azadmand Ali
Department of Pediatric Surgery, School of Medicine, Mashhad University of Medical Sciences, Sarvar Children's Hospital, Endoscopic and Minimally Invasive Surgery Research Center, Mashhad, Iran.
Department of Pediatric Anesthesiology, School of Medicine, Mashhad University of Medical Sciences, Sarvar Children's Hospital, Endoscopic and Minimally Invasive Surgery Research Center, Mashhad, Iran.
J Neonatal Surg. 2016 Jul 3;5(3):29. doi: 10.21699/jns.v5i3.344. eCollection 2016 Jul-Sep.
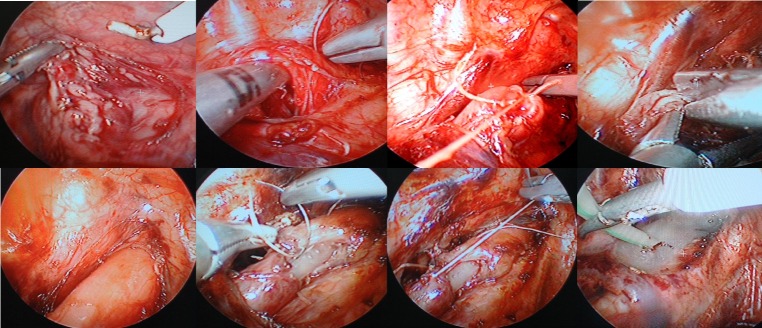
Thoracoscopic treatment of esophageal atresia and tracheoesophageal fistula (EA+TEF) is accepted as a superior technique at least in cosmetic point of view but it is considered as an advance endoscopic procedure that needs a learning curve to be performed perfectly. This is the first report of Iranian group pediatric surgeons in thoracoscopic approach to EA.
Since 2010, twenty four cases with EA+TEF underwent thoracoscopic approach in Sarvar Children Hospital (Mashhad -Iran). During the first 6 months, thoracoscopic approach to 6 cases of EA+TEF was converted to open procedure because of technical and instrumental problems. The first case of successful thoracoscopic EA repair was accomplished in 2010 and since then, 10 cases of EA+ TEF among 18 patients were treated successfully with thoracoscopic approach
Overall conversion rate was 58.3% but conversion rate after the primary learning curve period, was 35.7%. The main conversion causes include difficulties in esophageal anastomosis, limited exposure and deteriorating the patient's condition. Anastomotic leak and stenosis were observed in 20% and 40% respectively. Overall mortality rate was 4.2%.
Thoracoscopic repair of esophageal atresia seems feasible and safe with considerable superiorities to the conventional method although acceptable results needs a prolonged learning curve and advanced endoscopic surgical skill. Clear judgment about the best surgical intervention for EA according to all cosmetic and functional outcomes needs further studies.
胸腔镜治疗食管闭锁和食管气管瘘(EA+TEF)至少从美容角度被认为是一种更优的技术,但它被视为一种先进的内镜手术,需要经过学习曲线才能完美实施。这是伊朗小儿外科医生团队关于胸腔镜治疗EA的首次报告。
自2010年以来,24例EA+TEF患儿在伊朗马什哈德的萨瓦尔儿童医院接受了胸腔镜手术。在最初的6个月里,由于技术和器械问题,6例EA+TEF的胸腔镜手术转为开放手术。2010年完成了首例成功的胸腔镜下EA修复手术,从那时起,18例患者中的10例EA+TEF通过胸腔镜手术成功治疗。
总体转换率为58.3%,但在初步学习曲线期后的转换率为35.7%。主要的转换原因包括食管吻合困难、暴露受限和患者病情恶化。分别观察到吻合口漏和狭窄的发生率为20%和40%。总体死亡率为4.2%。
胸腔镜修复食管闭锁似乎是可行且安全的,与传统方法相比有相当大的优势,尽管要取得可接受的结果需要较长的学习曲线和先进的内镜手术技巧。根据所有美容和功能结果,对EA最佳手术干预的明确判断需要进一步研究。