Brown Benjamin, Cheraghi-Sohi Sudeh, Jaki Thomas, Su Ting-Li, Buchan Iain, Sperrin Matthew
Health eResearch Centre, Farr Institute, University of Manchester, Manchester, M13 9PL, UK.
NIHR Greater Manchester Primary Care Patient Safety Translational Research Centre, University of Manchester, Manchester, UK.
BMC Med Inform Decis Mak. 2016 Aug 9;16:106. doi: 10.1186/s12911-016-0343-y.
Well-designed clinical prediction models (CPMs) often out-perform clinicians at estimating probabilities of clinical outcomes, though their adoption by family physicians is variable. How family physicians interact with CPMs is poorly understood, therefore a better understanding and framing within a context-sensitive theoretical framework may improve CPM development and implementation. The aim of this study was to investigate why family physicians do or do not use CPMs, interpreting these findings within a theoretical framework to provide recommendations for the development and implementation of future CPMs.
Mixed methods study in North West England that comprised an online survey and focus groups.
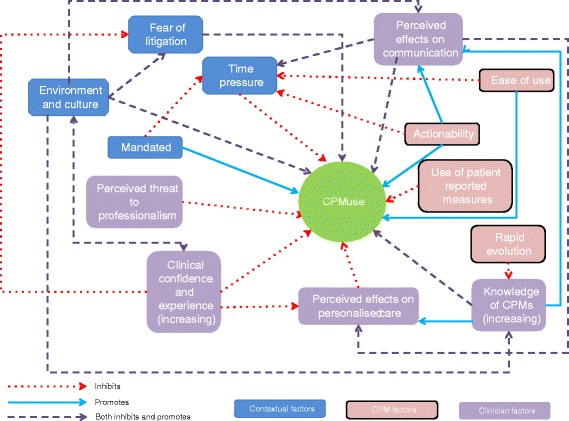
One hundred thirty eight respondents completed the survey, which found the main perceived advantages to using CPMs were that they guided appropriate treatment (weighted rank [r] = 299; maximum r = 414 throughout), justified treatment decisions (r = 217), and incorporated a large body of evidence (r = 156). The most commonly reported barriers to using CPMs were lack of time (r = 163), irrelevance to some patients (r = 161), and poor integration with electronic health records (r = 147). Eighteen clinicians participated in two focus groups (i.e. nine in each), which revealed 13 interdependent themes affecting CPM use under three overarching domains: clinician factors, CPM factors and contextual factors. Themes were interdependent, indicating the tensions family physicians experience in providing evidence-based care for individual patients.
The survey and focus groups showed that CPMs were valued when they supported clinical decision making and were robust. Barriers to their use related to their being time-consuming, difficult to use and not always adding value. Therefore, to be successful, CPMs should offer a relative advantage to current working, be easy to implement, be supported by training, policy and guidelines, and fit within the organisational culture.
设计良好的临床预测模型(CPMs)在估计临床结局概率方面通常比临床医生表现更优,尽管家庭医生对其采用情况参差不齐。目前对家庭医生与CPMs如何相互作用了解甚少,因此在一个情境敏感的理论框架内进行更好的理解和构建,可能会改善CPMs的开发和实施。本研究的目的是调查家庭医生使用或不使用CPMs的原因,并在理论框架内解读这些发现,为未来CPMs的开发和实施提供建议。
在英格兰西北部进行的混合方法研究,包括在线调查和焦点小组。
138名受访者完成了调查,结果发现使用CPMs的主要感知优势在于它们能指导适当的治疗(加权排名[r]=299;全程最大r=414)、为治疗决策提供依据(r=217)以及纳入大量证据(r=156)。最常报告的使用CPMs的障碍是缺乏时间(r=163)、与某些患者不相关(r=161)以及与电子健康记录整合不佳(r=147)。18名临床医生参加了两个焦点小组(即每组9人),揭示了在三个总体领域下影响CPMs使用的13个相互依存的主题:临床医生因素、CPMs因素和背景因素。这些主题相互依存,表明家庭医生在为个体患者提供循证护理时所经历的紧张关系。
调查和焦点小组表明,当CPMs支持临床决策且稳健时,它们受到重视。其使用障碍与耗时、难以使用以及并非总是能增加价值有关。因此,要取得成功,CPMs应在当前工作中具有相对优势,易于实施,得到培训、政策和指南的支持,并符合组织文化。