Department of Medicine, Division of Cardiology, Emory University School of Medicine, 101 Woodruff Circle, Woodruff Memorial Building, Atlanta, GA, 30322, USA.
Department of Biostatistics, School of Public Health, University of Alabama at Birmingham, Birmingham, AL, USA.
J Racial Ethn Health Disparities. 2017 Aug;4(4):718-724. doi: 10.1007/s40615-016-0275-3. Epub 2016 Aug 16.
Despite a higher prevalence of risk factors, atrial fibrillation (AF) is less prevalent in blacks than whites. To address this paradox, we examined racial differences in the magnitude of AF risk associated with common risk factors.
Participants (13,688; mean age = 63 ± 8.4 years; 56 % female; 37 % black) from the Reasons for Geographic And Racial Differences in Stroke study who were free of baseline AF were included. Incident AF was identified at a follow-up examination by electrocardiogram and self-reported medical history. Poisson regression was used to compute relative risk (RR) and 95 % confidence intervals (CI) for the association between risk factors and incident AF in blacks and whites, separately. Age- and sex-adjusted population attributable fractions (PAFs) of modifiable AF risk factors were computed.
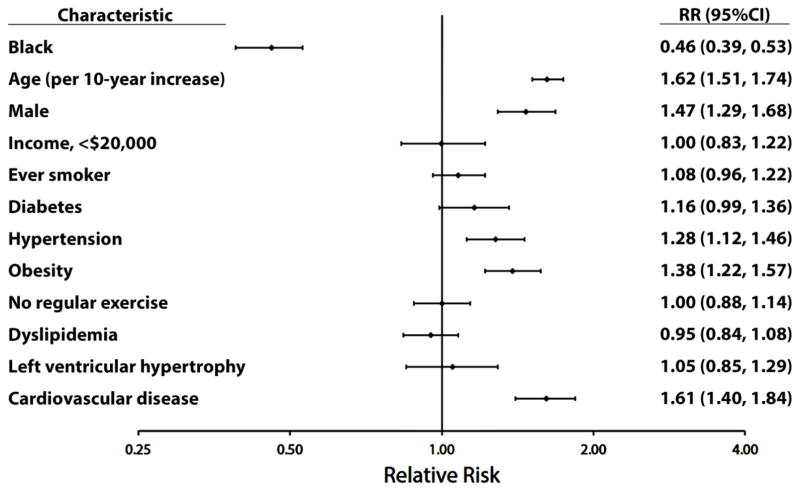
After median follow-up of 9.4 years, 997 (7.3 %) incident AF cases were detected. Black race was associated with a lower risk of AF (RR = 0.46, 95 % CI = 0.39, 0.53). Significant risk factors for AF were age, male sex, hypertension, obesity, and cardiovascular disease. A differential association was detected for smoking by race, with the association being stronger in blacks (RR = 1.41, 95 % CI = 1.07, 1.85) compared with whites (RR = 1.01, 95 % CI = 0.88, 1.16; P interaction = 0.030). The PAFs for hypertension (blacks = 27.4 %, whites = 19.4 %), obesity (blacks = 16.9 %, whites = 11.8 %), and smoking (blacks = 17.9 %, whites = 2.5 %) were higher for blacks than whites.
Modifiable risk factors are important in AF development among blacks despite a lower risk of the arrhythmia. Racial differences in the magnitude of the association of individual AF risk factors do not explain the AF paradox.
尽管黑人的风险因素患病率较高,但心房颤动 (AF) 的患病率却低于白人。为了解决这一矛盾,我们研究了与常见风险因素相关的 AF 风险的种族差异程度。
本研究纳入了 Reasons for Geographic And Racial Differences in Stroke 研究中的参与者(13688 人;平均年龄 63±8.4 岁;56%为女性;37%为黑人),这些参与者在基线时无 AF。通过心电图和自我报告的病史在随访检查中确定 AF 事件。分别使用泊松回归计算黑人与白人之间风险因素与 AF 事件之间的相对风险 (RR) 和 95%置信区间 (CI)。计算可改变的 AF 风险因素的年龄和性别调整人群归因分数 (PAF)。
中位随访 9.4 年后,检测到 997 例(7.3%)新发 AF 病例。黑人种族与 AF 风险降低相关(RR=0.46,95%CI=0.39,0.53)。AF 的显著风险因素包括年龄、男性、高血压、肥胖和心血管疾病。吸烟与种族之间存在差异关联,与白人相比,黑人的关联更强(RR=1.41,95%CI=1.07,1.85)(RR=1.01,95%CI=0.88,1.16;P 交互=0.030)。高血压(黑人 PAF=27.4%,白人 PAF=19.4%)、肥胖(黑人 PAF=16.9%,白人 PAF=11.8%)和吸烟(黑人 PAF=17.9%,白人 PAF=2.5%)的 PAF 在黑人中高于白人。
尽管 AF 风险较低,但可改变的风险因素在黑人的 AF 发展中很重要。个体 AF 风险因素的关联程度的种族差异并不能解释 AF 悖论。