Eldin Carole, Melenotte Cléa, Million Matthieu, Cammilleri Serge, Sotto Albert, Elsendoorn Antoine, Thuny Franck, Lepidi Hubert, Roblot France, Weitten Thierry, Assaad Souad, Bouaziz Anissa, Chapuzet Claire, Gras Guillaume, Labussiere Anne-Sophie, Landais Cécile, Longuet Pascale, Masseau Agathe, Mundler Olivier, Raoult Didier
Unité de Recherche sur les Maladies Infectieuses et Tropicales Emergentes, Faculté de Médecine, CNRS UMR 7278, IRD 198, Aix-Marseille Université, 27 Bd Jean Moulin Service de médecine nucléaire, Hôpital de La Timone, Marseille Service de pathologies infectieuses et tropicales de l'hôpital de Nimes Service de médecine, Hôpital de Chatellerault Unité Nord Insuffisance cardiaque et valvulopathies (UNIV), Service de cardiologie CHU de Marseille, Hôpital Nord, AP-HM Chemin des Bourrely, Marseille Service de Pathologies infectieuses et tropicales, CHU de Poitiers Service de Médecine interne Hôpital de Gap Service de Médecine interne, hôpital Saint Luc, Lyon Service de Rhumatologie, Centre hospitalier de Vienne Service de Pathologies infectieuses et tropicales, CHU de Rouen Service de Pathologies infectieuses et tropicales, CHU de Tours Service de Médecine Interne, CH de Bourges Service de Médecine Interne, Hôpital Saint-Anne, Toulon Service mobile d'Infectiologie, CH Victor Dupouy, Argenteuil Service de Médecine interne, CHU de Nantes, France.
Medicine (Baltimore). 2016 Aug;95(34):e4287. doi: 10.1097/MD.0000000000004287.
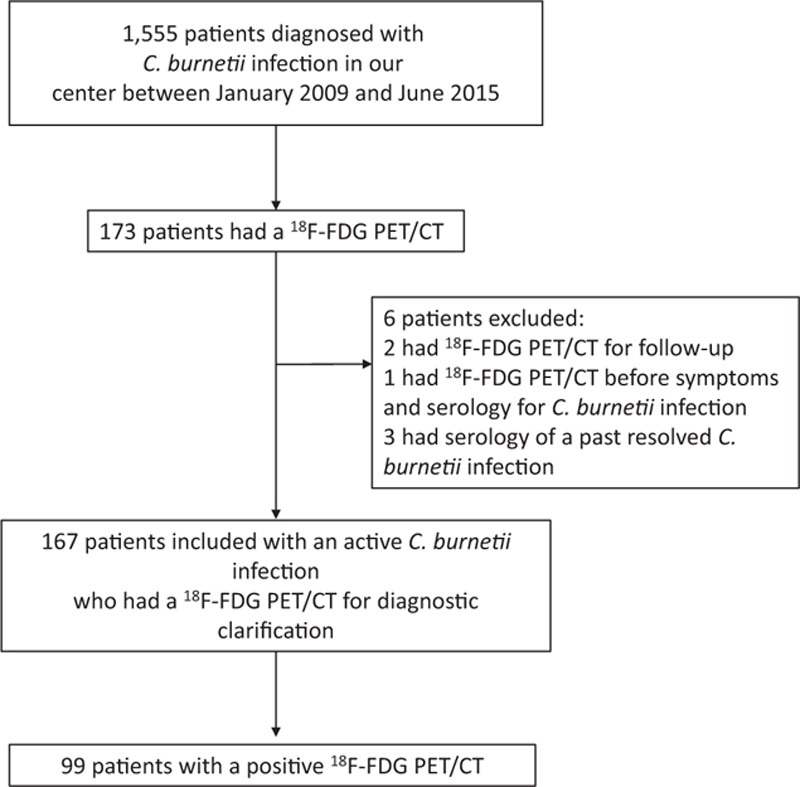
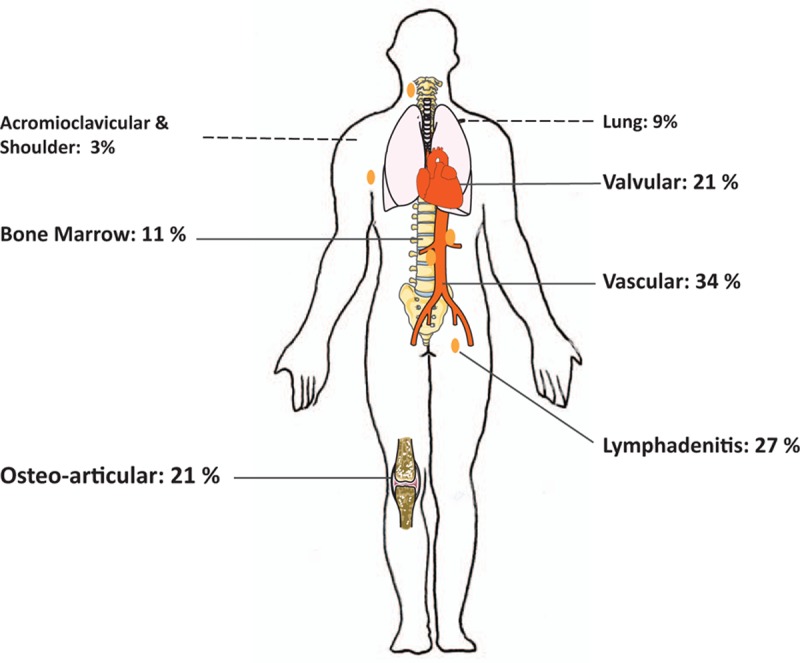
Because Q fever is mostly diagnosed serologically, localizing a persistent focus of Coxiella burnetii infection can be challenging. F-fluorodeoxyglucose positron emission tomography/computed tomography (F-FDG PET/CT) could be an interesting tool in this context.We performed a retrospective study on patients diagnosed with C burnetii infection, who had undergone F-FDG PET/CT between 2009 and 2015. When positive F-FDG PET/CT results were obtained, we tried to determine if it changed the previous diagnosis by discovering or confirming a suspected focus of C burnetii infection.One hundred sixty-seven patients benefited from F-FDG PET/CT. The most frequent clinical subgroup before F-FDG PET/CT was patients with no identified focus of infection, despite high IgG1 serological titers (34%). For 59% (n = 99) of patients, a hypermetabolic focus was identified. For 62 patients (62.6%), the positive F-FDG PET/CT allowed the diagnosis to be changed. For 24 of them, (38.7%), a previously unsuspected focus of infection was discovered. Forty-two (42%) positive patients had more than 1 hypermetabolic focus. We observed 21 valvular foci, 34 vascular foci, and a high proportion of osteoarticular localizations (n = 21). We also observed lymphadenitis (n = 27), bone marrow hypermetabolism (n = 11), and 9 pulmonary localizations.We confirmed thatF-FDG PET/CT is a central tool in the diagnosis of C burnetii focalized persistent infection. We proposed new diagnostic scores for 2 main clinical entities identified using F-FDG PET/CT: osteoarticular persistent infections and lymphadenitis.
由于Q热大多通过血清学诊断,因此定位伯纳特柯克斯体感染的持续病灶具有挑战性。在这种情况下,氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(F-FDG PET/CT)可能是一种有用的工具。我们对2009年至2015年间接受F-FDG PET/CT检查且被诊断为伯纳特柯克斯体感染的患者进行了一项回顾性研究。当获得阳性F-FDG PET/CT结果时,我们试图通过发现或确认疑似伯纳特柯克斯体感染病灶来确定其是否改变了先前的诊断。167例患者接受了F-FDG PET/CT检查。F-FDG PET/CT检查前最常见的临床亚组是尽管IgG1血清学滴度很高但未发现感染病灶的患者(34%)。59%(n = 99)的患者发现了代谢亢进病灶。62例患者(62.6%)的阳性F-FDG PET/CT结果使诊断得以改变。其中24例(38.7%)发现了先前未怀疑的感染病灶。42例(42%)阳性患者有不止1个代谢亢进病灶。我们观察到21个瓣膜病灶、34个血管病灶以及高比例的骨关节炎定位(n = 21)。我们还观察到淋巴结炎(n = 27)、骨髓代谢亢进(n = 11)和9个肺部定位。我们证实F-FDG PET/CT是诊断伯纳特柯克斯体局限性持续感染的核心工具。我们针对使用F-FDG PET/CT识别出的2个主要临床实体提出了新的诊断评分:骨关节炎持续感染和淋巴结炎。