Mohammad Hasan Raza, Boardman Jeremy, Howell Laura, Mills Roger J, Emsley Hedley C A
Department of Neurology, Royal Preston Hospital, Sharoe Green Lane, Fulwood, Preston, PR2 9HT, UK.
Faculty of Biology, Medicine and Health, University of Manchester, Oxford Road, Manchester, M13 9PL, UK.
BMC Neurol. 2016 Aug 26;16(1):152. doi: 10.1186/s12883-016-0677-1.
Urgent referral for suspected central nervous system (CNS) cancer is recommended, but little analysis of the referral criteria diagnostic performance has been conducted. New 2015 NICE guidance recommends direct brain imaging for patients with symptoms with positive predictive values (PPV) of 3 %, but further guidance is needed.
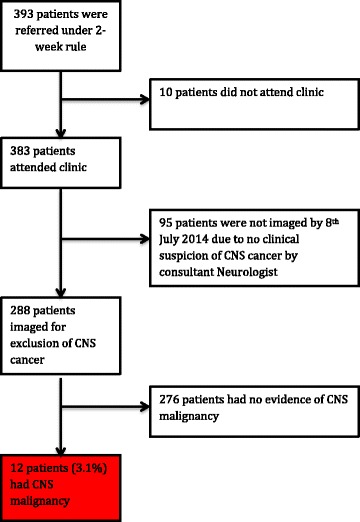
A 12-month retrospective evaluation of 393 patients referred under previous 2005 NICE 2-week rule criteria was conducted. Analysis was based on the three groups of symptoms forming the referral criteria, (1) CNS symptoms, (2) recent onset headaches, (3) rapidly progressive subacute focal deficit/cognitive/behavioural/personality change. Comparison was made with neuroimaging findings.
Twelve (3.1 %) of 383 patients who attended clinic had CNS cancer suggesting the combination of clinical judgement and application of 2005 criteria matched the 2015 guideline's PPV threshold. PPVs for the three groups of symptoms were (1) 4.1 % (95 % CIs 2.0 to 7.4 %), (2) 1.2 % (0.1 to 4.3 %) and (3) 3.7 % (0.1 to 19.0 %). Sensitivities were (1) 83.3 % (95 % CIs 51.6 to 97.9 %), (2) 16.7 % (2.1 to 48.4 %), and (3) 8.3 % (0.2 to 38.5 %); specificities were (1) 37.2 % (32.3 to 42.3 %), (2) 55.5 % (50.3 to 60.7 %) and (3) 93.0 % (89.9 to 95.4 %). Of 288 patients who underwent neuroimaging, 59 (20.5 %) had incidental findings, most commonly cerebrovascular disease.
The 2015 guidance is less prescriptive than previous criteria making clinical judgement more important. CNS symptoms had greatest sensitivity, while PPVs for CNS symptoms and rapidly progressive subacute deficit/cognitive/behavioural/personality change were closest to 3 %. Recent onset headaches had the lowest sensitivity and PPV.
对于疑似中枢神经系统(CNS)癌症患者,建议进行紧急转诊,但对转诊标准诊断性能的分析较少。2015年英国国家卫生与临床优化研究所(NICE)的新指南建议对有症状的患者进行直接脑部成像,其阳性预测值(PPV)为3%,但还需要进一步的指导。
对393例根据2005年NICE两周规则标准转诊的患者进行了为期12个月的回顾性评估。分析基于构成转诊标准的三组症状:(1)中枢神经系统症状;(2)近期发作的头痛;(3)快速进展的亚急性局灶性缺损/认知/行为/人格改变。并与神经影像学检查结果进行比较。
383例到诊所就诊的患者中有12例(3.1%)患有中枢神经系统癌症,这表明临床判断与2005年标准的应用相结合符合了2015年指南的PPV阈值。三组症状的PPV分别为:(1)4.1%(95%置信区间2.0%至7.4%);(2)1.2%(0.1%至4.3%);(3)3.7%(0.1%至19.0%)。敏感性分别为:(1)83.3%(95%置信区间51.6%至97.9%);(2)16.7%(2.1%至48.4%);(3)8.3%(0.2%至38.5%);特异性分别为:(1)37.2%(32.3%至42.3%);(2)55.5%(50.3%至60.7%);(3)93.(89.9%至95.4%)。在288例接受神经影像学检查的患者中,59例(20.5%)有意外发现,最常见的是脑血管疾病。
2015年的指南比以前的标准规定性更低,使得临床判断更为重要。中枢神经系统症状的敏感性最高,而中枢神经系统症状和快速进展的亚急性缺损/认知/行为/人格改变的PPV最接近3%。近期发作的头痛敏感性和PPV最低。