Translational Neurosurgery, Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, UK.
University of Edinburgh Medical School, Edinburgh, UK.
BMC Fam Pract. 2019 Aug 20;20(1):118. doi: 10.1186/s12875-019-1003-y.
Brain tumour patients see their primary care doctor on average three or more times before diagnosis, so there may be an opportunity to identify 'at risk' patients earlier. Suspecting a brain tumour diagnosis is difficult because brain tumour-related symptoms are typically non-specific.
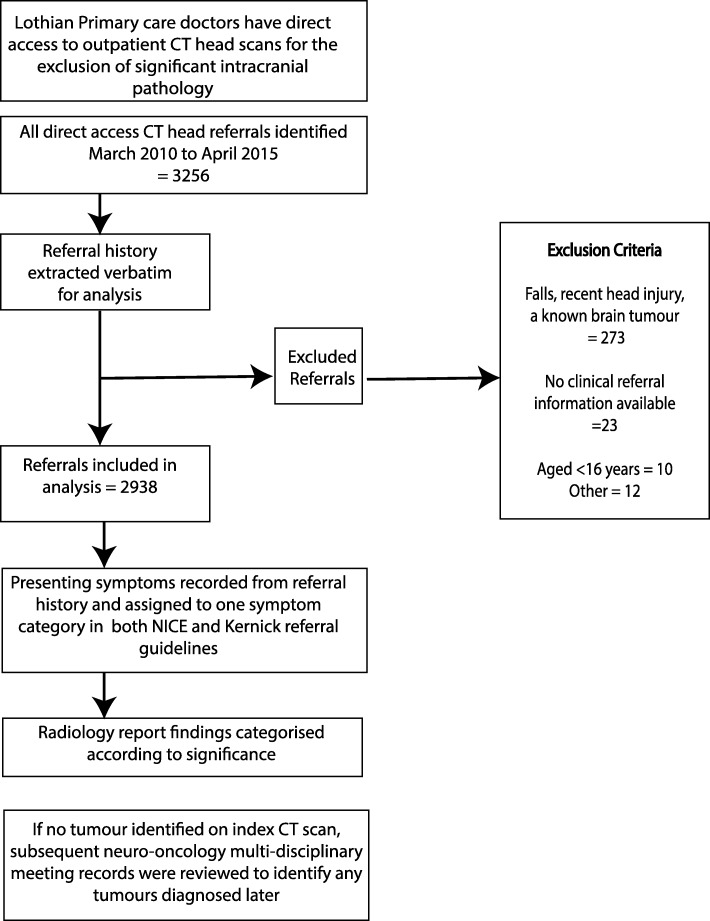
We explored the predictive value of referral guidelines (Kernick and NICE 2005) for brain imaging where a tumour is suspected, in a population-based patient group referred for direct access CT of the head. A consensus panel reviewed whether non-tumour findings were clinically important or whether further investigation was necessary.
Over a 5-year period, 3257 head scans were performed; 318 scans were excluded according to pre-specified criteria. 53 patients (1.8%) were reported to have intracranial tumours, of which 42 were significant (diagnostic yield of 1.43%). There were no false negative CT scans for tumour. With symptom-based referral guidelines primary care doctors can identify patients with a 3% positive predictive value (PPV). 559 patients had non-tumour findings, 31% of which were deemed clinically significant. In 34% of these 559 patients, referral for further imaging and/or specialist assessment from primary care was still thought warranted.
Existing referral guidelines are insufficient to stratify patients adequately based on their symptoms, according to the likelihood that a tumour will be found on brain imaging. Identification of non-tumour findings may be significant for patients and earlier specialist input into interpretation of these images may be beneficial. Improving guidelines to better identify patients at risk of a brain tumour should be a priority, to improve speed of diagnosis, and reduce unnecessary imaging and costs. Future guidelines may incorporate groups of symptoms, clinical signs and tests to improve the predictive value.
脑肿瘤患者在确诊前平均会看 3 次或更多次初级保健医生,因此可能有机会更早地识别出“高危”患者。怀疑脑肿瘤诊断很困难,因为脑肿瘤相关症状通常是非特异性的。
我们在一个因疑似脑肿瘤而被直接转介行头部 CT 检查的患者群体中,探索了转诊指南(Kernick 和 NICE 2005)对疑似脑肿瘤患者进行脑成像的预测价值。共识小组审查了非肿瘤发现是否具有临床意义,或者是否需要进一步检查。
在 5 年期间,进行了 3257 次头部扫描;根据预先规定的标准排除了 318 次扫描。报告有颅内肿瘤的患者有 53 例(1.8%),其中 42 例为显著肿瘤(诊断率为 1.43%)。没有肿瘤的假阴性 CT 扫描。根据基于症状的转诊指南,初级保健医生可以识别出具有 3%阳性预测值(PPV)的患者。有 559 例患者有非肿瘤发现,其中 31%被认为具有临床意义。在这 559 例患者中的 34%中,仍认为需要从初级保健转介进行进一步成像和/或专家评估。
根据在脑成像上发现肿瘤的可能性,现有的转诊指南不足以根据患者的症状充分分层。识别非肿瘤发现可能对患者具有重要意义,并且早期由专家参与解释这些图像可能会受益。优先改善指南以更好地识别患有脑肿瘤风险的患者,应有助于提高诊断速度,并减少不必要的影像学检查和费用。未来的指南可能会纳入一组症状、临床体征和检查,以提高预测价值。