Guo Zhiliang, Yu Shuhong, Xiao Lulu, Chen Xin, Ye Ruidong, Zheng Ping, Dai Qiliang, Sun Wen, Zhou Changsheng, Wang Shuiping, Zhu Wusheng, Liu Xinfeng
Department of Neurology, Jinling Hospital, Medical School of Nanjing University, 305 E Zhongshan Rd, Nanjing, 210002, Jiangsu Province, China.
Department of Neurology, Second Affiliated Hospital of Soochow University, Suzhou, 215004, China.
J Neuroinflammation. 2016 Aug 26;13(1):199. doi: 10.1186/s12974-016-0680-x.
The neutrophil to lymphocyte ratio (NLR) has been shown to predict short- and long-term outcomes in ischemic stroke patients. We sought to explore the temporal profile of the plasma NLR in stroke patients treated with intravenous thrombolysis (IVT) and its relationship with intracranial bleeding complications after thrombolysis.
A total of 189 ischemic stroke patients were prospectively enrolled. Blood samples for leukocyte, neutrophil, and lymphocyte counts were obtained at admission and at 3-6, 12-18, and 36-48 h after IVT. Head CT was performed on admission and repeated after 36-48 h, and a CT scan was done immediately in case of clinical worsening. Hemorrhagic events were categorized as symptomatic intracranial hemorrhage (sICH) and parenchymal hematomas (PH) according to previously published criteria.
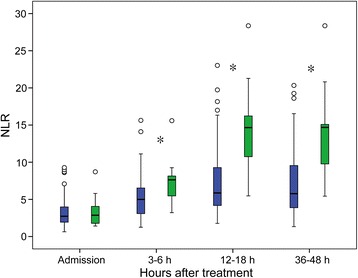
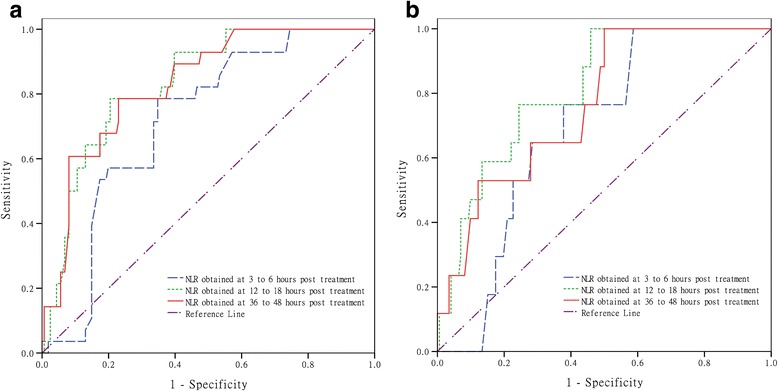
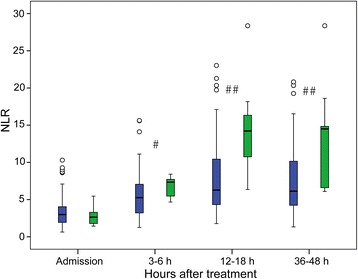
An increasing trend in the NLR was observed after stroke, and the NLR was higher in patients who developed PH or sICH at 3-6, 12-18, and 36-48 h after IVT (P < 0.01) than in those without PH or sICH. The optimal cutoff value for the serum NLR as an indicator for auxiliary diagnosis of PH and sICH was 10.59 at 12-18 h. Furthermore, the NLR obtained at 12-18-h post-treatment was independently associated with PH (adjusted odds ratio [OR] 1.14) and sICH (adjusted OR 1.14). In addition, patients with a NLR ≥10.59 had an 8.50-fold greater risk for PH (95 % confidence interval [CI] 2.69-26.89) and a 7.93-fold greater risk for sICH (95 % CI 2.25-27.99) than patients with a NLR <10.59.
NLR is a dynamic variable, and its variation is associated with HT after thrombolysis in stroke patients.
中性粒细胞与淋巴细胞比值(NLR)已被证明可预测缺血性中风患者的短期和长期预后。我们试图探讨接受静脉溶栓(IVT)治疗的中风患者血浆NLR的时间变化情况及其与溶栓后颅内出血并发症的关系。
前瞻性纳入189例缺血性中风患者。在入院时以及IVT后3 - 6、12 - 18和36 - 48小时采集白细胞、中性粒细胞和淋巴细胞计数的血样。入院时进行头部CT检查,并在36 - 48小时后复查,如临床症状恶化则立即进行CT扫描。根据先前公布的标准,将出血事件分为症状性颅内出血(sICH)和实质性血肿(PH)。
中风后观察到NLR呈上升趋势,在IVT后3 - 6、12 - 18和36 - 48小时发生PH或sICH的患者的NLR高于未发生PH或sICH的患者(P < 0.01)。血清NLR作为辅助诊断PH和sICH的指标,在12 - 18小时的最佳截断值为10.59。此外,治疗后12 - 18小时获得的NLR与PH(调整后的优势比[OR] 1.14)和sICH(调整后的OR 1.14)独立相关。此外,NLR≥10.59的患者发生PH的风险比NLR < 10.59的患者高8.50倍(95%置信区间[CI] 2.69 - 26.89),发生sICH的风险高7.93倍(95% CI 2.25 - 27.99)。
NLR是一个动态变量,其变化与中风患者溶栓后的颅内出血相关。