Yovich John L, Alsbjerg Birgit, Conceicao Jason L, Hinchliffe Peter M, Keane Kevin N
PIVET Medical Centre, Perth; School of Biomedical Science, Curtin Health Innovation Research Institute Bioscience, Curtin University, Perth, WA, Australia.
The Fertility Clinic, Skive Regional Hospital, Skive; Faculty of Health, Aarhus University, Aarhus, Denmark.
Drug Des Devel Ther. 2016 Aug 10;10:2561-73. doi: 10.2147/DDDT.S104104. eCollection 2016.
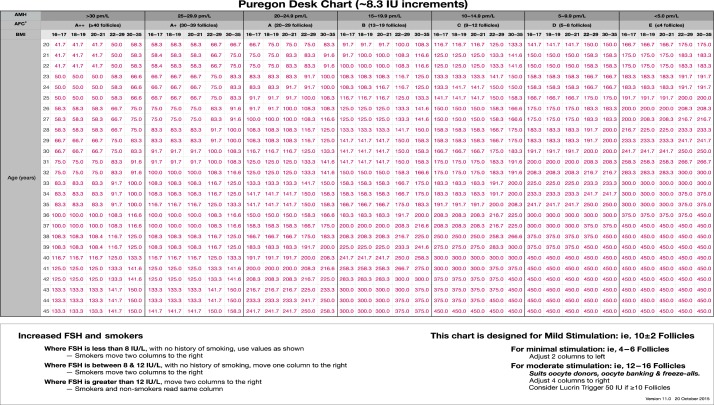
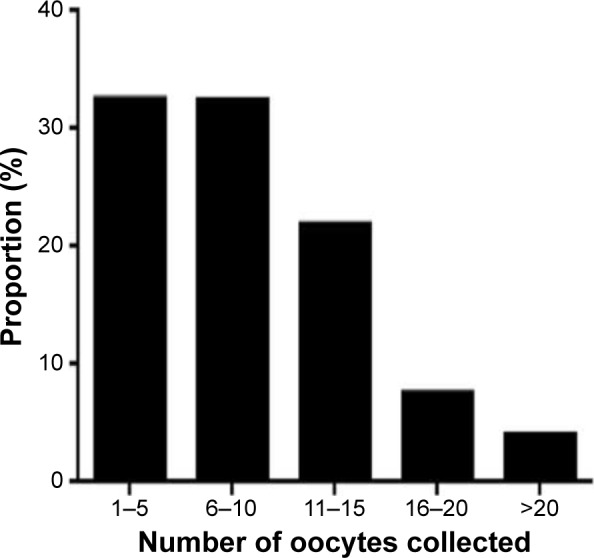
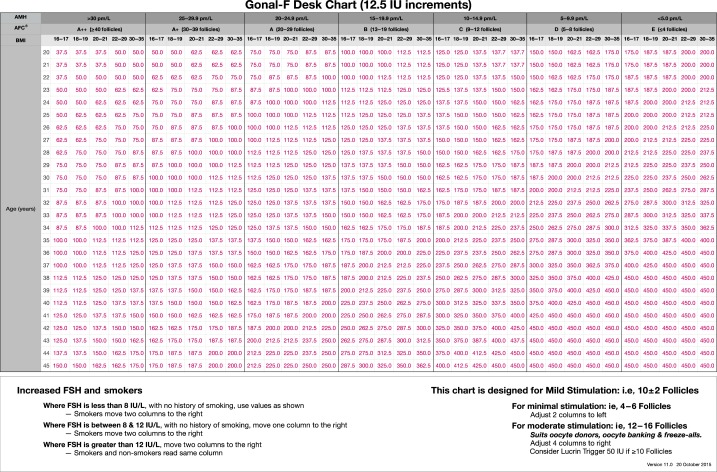
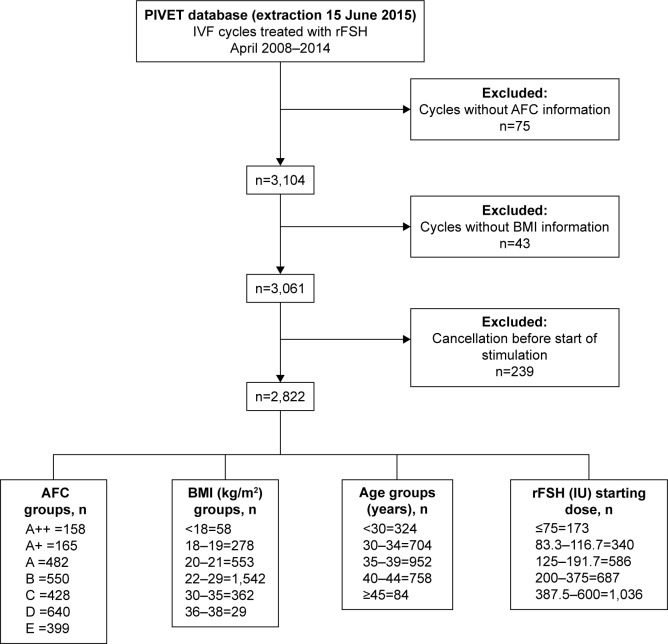
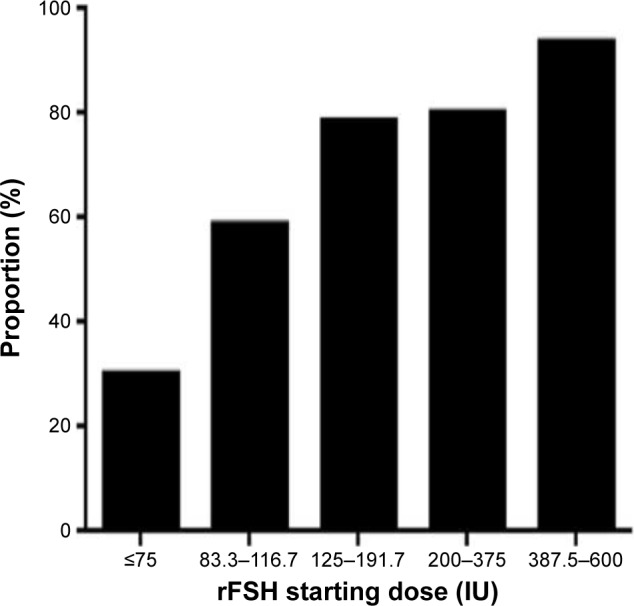
The first PIVET algorithm for individualized recombinant follicle stimulating hormone (rFSH) dosing in in vitro fertilization, reported in 2012, was based on age and antral follicle count grading with adjustments for anti-Müllerian hormone level, body mass index, day-2 FSH, and smoking history. In 2007, it was enabled by the introduction of a metered rFSH pen allowing small dosage increments of ~8.3 IU per click. In 2011, a second rFSH pen was introduced allowing more precise dosages of 12.5 IU per click, and both pens with their individual algorithms have been applied continuously at our clinic. The objective of this observational study was to validate the PIVET algorithms pertaining to the two rFSH pens with the aim of collecting ≤15 oocytes and minimizing the risk of ovarian hyperstimulation syndrome. The data set included 2,822 in vitro fertilization stimulations over a 6-year period until April 2014 applying either of the two individualized dosing algorithms and corresponding pens. The main outcome measures were mean oocytes retrieved and resultant embryos designated for transfer or cryopreservation permitted calculation of oocyte and embryo utilization rates. Ensuing pregnancies were tracked until live births, and live birth productivity rates embracing fresh and frozen transfers were calculated. Overall, the results showed that mean oocyte numbers were 10.0 for all women <40 years with 24% requiring rFSH dosages <150 IU. Applying both specific algorithms in our clinic meant that the starting dose was not altered for 79.1% of patients and for 30.1% of those receiving the very lowest rFSH dosages (≤75 IU). Only 0.3% patients were diagnosed with severe ovarian hyperstimulation syndrome, all deemed avoidable due to definable breaches from the protocols. The live birth productivity rates exceeded 50% for women <35 years and was 33.2% for the group aged 35-39 years. Routine use of both algorithms led to only 11.6% of women generating >15 oocytes, significantly lower than recently published data applying conventional dosages (38.2%; P<0.0001). When comparing both specific algorithms to each other, the outcomes were mainly comparable for pregnancy, live birth, and miscarriage rate. However, there were significant differences in relation to number of oocytes retrieved, but the mean for both the algorithms remained well below 15 oocytes. Consequently, application of both these algorithms in our in vitro fertilization clinic allows the use of both the rFSH products, with very similar results, and they can be considered validated on the basis of effectiveness and safety, clearly avoiding ovarian hyperstimulation syndrome.
2012年报道的首个用于体外受精中个体化重组促卵泡激素(rFSH)给药的PIVET算法,是基于年龄和窦卵泡计数分级,并根据抗苗勒管激素水平、体重指数、第2天的促卵泡激素水平和吸烟史进行调整。2007年,计量rFSH笔的推出使得该算法得以应用,每次点击可实现约8.3 IU的小剂量增加。2011年,推出了第二种rFSH笔,每次点击可实现更精确的12.5 IU剂量,这两种笔及其各自的算法在我们诊所持续应用。这项观察性研究的目的是验证与这两种rFSH笔相关的PIVET算法,目标是采集≤15个卵母细胞并将卵巢过度刺激综合征的风险降至最低。数据集包括在截至2014年4月的6年期间应用两种个体化给药算法及相应笔进行的2822次体外受精刺激。主要结局指标是回收的平均卵母细胞数以及用于移植或冷冻保存的所得胚胎,据此可计算卵母细胞和胚胎利用率。追踪后续妊娠直至活产,并计算包括新鲜移植和冷冻移植的活产生产率。总体而言,结果显示所有年龄<40岁的女性平均卵母细胞数为10.0个,24%的女性需要的rFSH剂量<150 IU。在我们诊所应用这两种特定算法意味着79.1%的患者起始剂量未改变,对于接受极低rFSH剂量(≤75 IU)的患者,这一比例为30.1%。仅0.3%的患者被诊断为重度卵巢过度刺激综合征,所有这些病例因可明确的方案违规被认为是可避免的。年龄<35岁的女性活产生产率超过50%,35 - 39岁组为33.2%。常规使用这两种算法导致仅11.6%的女性产生>15个卵母细胞,显著低于最近发表的应用传统剂量的数据(38.2%;P<0.0001)。当将这两种特定算法相互比较时,妊娠、活产和流产率的结果主要具有可比性。然而,在回收的卵母细胞数量方面存在显著差异,但两种算法的平均值仍远低于15个卵母细胞。因此,在我们的体外受精诊所应用这两种算法可使用这两种rFSH产品,结果非常相似,并且基于有效性和安全性可认为它们得到了验证,明显避免了卵巢过度刺激综合征。