Byhoff Elena, Harris John A, Langa Kenneth M, Iwashyna Theodore J
Department of Medicine, University of Michigan, Ann Arbor, Michigan.
Robert Wood Johnson Foundation Clinical Scholars Program, University of Michigan, Ann Arbor, Michigan.
J Am Geriatr Soc. 2016 Sep;64(9):1789-97. doi: 10.1111/jgs.14263. Epub 2016 Sep 1.
To determine to what extent demographic, social support, socioeconomic, geographic, medical, and End-of-Life (EOL) planning factors explain racial and ethnic variation in Medicare spending during the last 6 months of life.
Retrospective cohort study.
Health and Retirement Study (HRS).
Decedents who participated in HRS between 1998 and 2012 and previously consented to survey linkage with Medicare claims (N = 7,105).
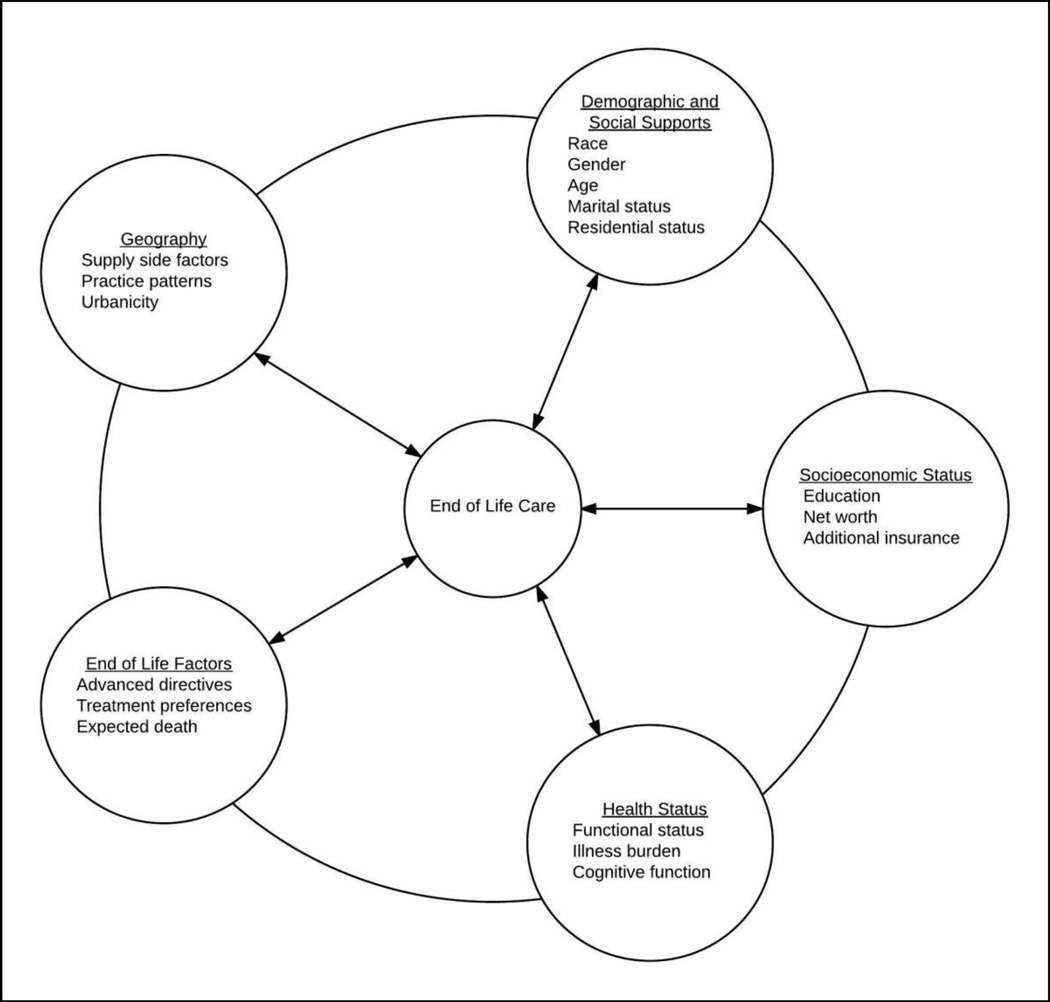
Total Medicare expenditures in the last 180 days of life according to race and ethnicity, controlling for demographic factors, social supports, geography, illness burden, and EOL planning factors, including presence of advance directives, discussion of EOL treatment preferences, and whether death had been expected.
The analysis included 5,548 (78.1%) non-Hispanic white, 1,030 (14.5%) non-Hispanic black, and 331 (4.7%) Hispanic adults and 196 (2.8%) adults of other race or ethnicity. Unadjusted results suggest that average EOL Medicare expenditures were $13,522 (35%, P < .001) more for black decedents and $16,341 (42%, P < .001) more for Hispanics than for whites. Controlling for demographic, socioeconomic, geographic, medical, and EOL-specific factors, the Medicare expenditure difference between groups fell to $8,047 (22%, P < .001) more for black and $6,855 (19%, P < .001) more for Hispanic decedents than expenditures for non-Hispanic whites. The expenditure differences between groups remained statistically significant in all models.
Individuals-level factors, including EOL planning factors do not fully explain racial and ethnic differences in Medicare spending in the last 6 months of life. Future research should focus on broader systemic, organizational, and provider-level factors to explain these differences.
确定人口统计学、社会支持、社会经济、地理、医疗及临终(EOL)规划因素在多大程度上能够解释临终前6个月医疗保险支出中的种族和民族差异。
回顾性队列研究。
健康与退休研究(HRS)。
1998年至2012年间参与HRS且之前同意将调查与医疗保险理赔数据相链接的逝者(N = 7105)。
根据种族和民族划分,在控制人口统计学因素、社会支持、地理位置、疾病负担及EOL规划因素(包括生前预嘱的存在、临终治疗偏好的讨论以及死亡是否可预期)的情况下,计算临终前180天的医疗保险总支出。
分析纳入了5548名(78.1%)非西班牙裔白人、1030名(14.5%)非西班牙裔黑人、331名(4.7%)西班牙裔成年人以及196名(2.8%)其他种族或民族的成年人。未经调整的结果显示,黑人逝者的临终医疗保险平均支出比白人多13522美元(35%,P <.001),西班牙裔比白人多16341美元(42%,P <.001)。在控制了人口统计学、社会经济、地理、医疗及EOL特定因素后,黑人和西班牙裔逝者的医疗保险支出与非西班牙裔白人相比,分别多出8047美元(22%,P <.001)和6855美元(19%,P <.001)。在所有模型中,组间支出差异均具有统计学意义。
个体层面的因素,包括EOL规划因素,并不能完全解释临终前6个月医疗保险支出中的种族和民族差异。未来的研究应聚焦于更广泛的系统、组织及提供者层面的因素来解释这些差异。