Shirakabe Akihiro, Kobayashi Nobuaki, Hata Noritake, Shinada Takuro, Tomita Kazunori, Tsurumi Masafumi, Okazaki Hirotake, Matsushita Masato, Yamamoto Yoshiya, Yokoyama Shinya, Asai Kuniya, Shimizu Wataru
Division of Intensive Care Unit, Nippon Medical School Chiba Hokusoh Hospital, 1715 Kamagari, Inzai, Chiba, 270-1694, Japan.
Department of Cardiovascular Medicine, Nippon Medical School, Tokyo, Japan.
BMC Cardiovasc Disord. 2016 Sep 5;16(1):174. doi: 10.1186/s12872-016-0340-1.
No cardiac biomarkers for detecting acute kidney injury (AKI) on admission in non-surgical intensive care patients have been reported. The aim of the present study is to elucidate the role of cardiac biomarkers for quickly identifying the presence of AKI on admission.
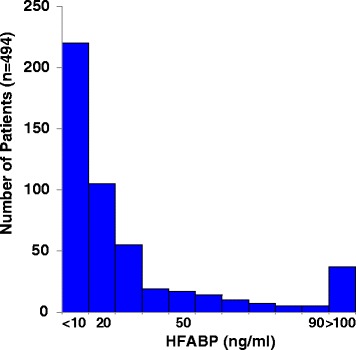
Data for 1183 patients who underwent the measurement of cardiac biomarkers, including the serum heart-type fatty acid-binding protein (s-HFABP) level, in the emergency department were screened, and 494 non-surgical intensive care patients were enrolled in this study. Based on the RIFLE classification, which was the ratio of the serum creatinine value recorded on admission to the baseline creatinine value, the patients were assigned to a no-AKI (n = 349) or AKI (Class R [n = 83], Class I [n = 36] and Class F [n = 26]) group on admission. We evaluated the diagnostic value of the s-H-FABP level for detecting AKI and Class I/F. The mid-term prognosis, as all-cause death within 180 days, was also evaluated.
The s-H-FABP levels were significantly higher in the Class F (79.2 [29.9 to 200.3] ng/mL) than in the Class I (41.5 [16.7 to 71.6] ng/mL), the Class R (21.1 [10.2 to 47.9] ng/mL), and no-AKI patients (8.8 [5.4 to 17.7] ng/mL). The most predictive values for detecting AKI were Q2 (odds ratio [OR]: 3.743; 95 % confidence interval [CI]: 1.693-8.274), Q3 (OR: 9.427; 95 % CI: 4.124-21.548), and Q4 (OR: 28.000; 95 % CI: 11.245-69.720), while those for Class I/F were Q3 (OR: 5.155; 95 % CI: 1.030-25.790) and Q4 (OR: 22.978; 95 % CI: 4.814-109.668). The s-HFABP level demonstrating an optimal balance between sensitivity and specificity (70.3 and 72.8 %, respectively; area under the curve: 0.774; 95 % CI: 0.728-0.819) was 15.7 ng/mL for AKI and 20.7 ng/mL for Class I/F (71.0 and 83.1 %, respectively; area under the curve: 0.818; 95 % CI: 0.763-0.873). The prognosis was significantly poorer in the high serum HFABP with AKI group than in the other groups.
The s-H-FABP level is an effective biomarker for detecting AKI in non-surgical intensive care patients.
尚无关于非手术重症监护患者入院时检测急性肾损伤(AKI)的心脏生物标志物的报道。本研究旨在阐明心脏生物标志物在快速识别入院时AKI存在情况中的作用。
筛选了1183例在急诊科接受心脏生物标志物检测(包括血清心型脂肪酸结合蛋白[s-HFABP]水平)的患者的数据,494例非手术重症监护患者纳入本研究。根据RIFLE分类(即入院时记录的血清肌酐值与基线肌酐值之比),将患者分为入院时无AKI组(n = 349)或AKI组(R级[n = 83]、I级[n = 36]和F级[n = 26])。我们评估了s-H-FABP水平对检测AKI和I/F级的诊断价值。还评估了中期预后,即180天内的全因死亡情况。
F级患者的s-H-FABP水平(79.2[29.9至200.3]ng/mL)显著高于I级患者(41.5[16.7至71.6]ng/mL)、R级患者(21.1[10.2至47.9]ng/mL)和无AKI患者(8.8[5.4至17.7]ng/mL)。检测AKI的最具预测价值的指标是Q2(比值比[OR]:3.743;95%置信区间[CI]:1.693 - 8.274)、Q3(OR:9.427;95%CI:4.124 - 21.548)和Q4(OR:28.000;95%CI:11.245 - 69.720),而检测I/F级的指标是Q3(OR:5.155;95%CI:1.030 - 25.790)和Q4(OR:22.978;95%CI:4.814 - 109.668)。对于AKI,在敏感性和特异性之间表现出最佳平衡(分别为70.3%和72.8%;曲线下面积:0.774;95%CI:0.728 - 0.819)的s-HFABP水平为15.7 ng/mL,对于I/F级为20.7 ng/mL(分别为71.0%和83.1%;曲线下面积:0.818;95%CI:0.763 - 0.873)。高血清HFABP合并AKI组的预后明显比其他组差。
s-H-FABP水平是检测非手术重症监护患者AKI的有效生物标志物。