Presseau Justin, Grimshaw Jeremy M, Tetroe Jacqueline M, Eccles Martin P, Francis Jill J, Godin Gaston, Graham Ian D, Hux Janet E, Johnston Marie, Légaré France, Lemyre Louise, Robinson Nicole, Zwarenstein Merrick
Ottawa Hospital Research Institute, The Ottawa Hospital, General Campus, 501 Smyth Road, Box 201B, Ottawa, Ontario, K1H 8L6, Canada.
School of Epidemiology, Public Health and Preventive Medicine, 451 Smyth Road, Ottawa, Ontario, K1H 8M5, Canada.
Implement Sci. 2016 Sep 13;11(1):121. doi: 10.1186/s13012-016-0485-4.
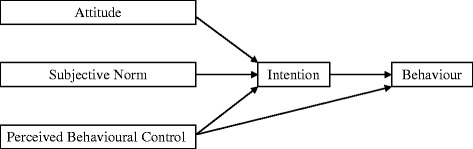
Pragmatic trials of implementation interventions focus on evaluating whether an intervention changes professional behaviour under real-world conditions rather than investigating the mechanism through which change occurs. Theory-based process evaluations conducted alongside pragmatic randomised trials address this by assessing whether the intervention changes theoretical constructs proposed to mediate change. The Ontario Printed Educational Materials (PEM) cluster trial was designed to increase family physicians' guideline-recommended prescription of thiazide diuretics. The trial found no intervention effect. Using the theory of planned behaviour (TPB), we hypothesised that changes in thiazide prescribing would be reflected in changes in intention, consistent with changes in attitude and subjective norm, with no change to their perceived behavioural control (PBC), and tested this alongside the RCT.
We developed and sent TPB postal questionnaires to a random sub-sample of family physicians in each trial arm 2 months before and 6 months after dissemination of the PEMs. We used analysis of covariance to test for group differences using a 2 × 3 factorial design. We content-analysed an open-ended question about perceived barriers to thiazide prescription. Using control group data, we tested whether baseline measures of TPB constructs predicted self-reported thiazide prescribing at follow-up.
Four hundred twenty-six physicians completed pre- and post-intervention questionnaires. Baseline scores on measures of TPB constructs were high: intention mean = 5.9 out of 7 (SD = 1.4), attitude mean = 5.8 (SD = 1.1), subjective norm mean = 5.8 (SD = 1.1) and PBC mean = 6.2 (SD = 1.0). The arms did not significantly differ post-intervention on any of the theory-based constructs, suggesting a possible ceiling effect. Content analysis of perceived barriers suggested post-intentional barriers to prescribing thiazides most often focused on specific patient clinical characteristics and potential side effects. Baseline intention (β = 0.63, p < 0.01) but not PBC (β = 0.04, p = 0.78) predicted 42.6 % of the variance in self-reported behaviour at follow-up in the control group.
Congruent with the Ontario Printed Educational Messages trial results and aligned with the TPB, we saw no impact of the intervention on any TPB constructs. The theoretical basis of this evaluation suggests possible explanations for the failure of the PEM intervention to change professional behaviour, which can directly inform the design and content of future theory-based PEM interventions to change professional behaviour.
ISRCTN, Canada ISRCTN72772651.
实施干预措施的实用性试验侧重于评估干预措施在现实世界条件下是否能改变专业行为,而非探究改变发生的机制。与实用性随机试验同时进行的基于理论的过程评估通过评估干预措施是否能改变为介导变化而提出的理论结构来解决这一问题。安大略省印刷教育材料(PEM)整群试验旨在增加家庭医生按照指南推荐使用噻嗪类利尿剂的处方量。该试验未发现干预效果。我们运用计划行为理论(TPB)假设,噻嗪类药物处方的变化会反映在意向的变化中,这与态度和主观规范的变化一致,而其感知行为控制(PBC)不变,并在随机对照试验中对此进行了检验。
在PEM传播前2个月和传播后6个月,我们向每个试验组的家庭医生随机子样本发放并邮寄TPB问卷。我们采用协方差分析,使用2×3析因设计来检验组间差异。我们对一个关于噻嗪类药物处方感知障碍的开放式问题进行了内容分析。利用对照组数据,我们检验了TPB结构的基线测量值是否能预测随访时自我报告的噻嗪类药物处方情况。
426名医生完成了干预前后的问卷。TPB结构测量的基线分数较高:意向平均分为7分中的5.9分(标准差=1.4),态度平均分为5.8分(标准差=1.1),主观规范平均分为5.8分(标准差=1.1),PBC平均分为6.2分(标准差=1.0)。干预后,各试验组在任何基于理论的结构上均无显著差异,这表明可能存在天花板效应。对感知障碍的内容分析表明,噻嗪类药物处方的意向后障碍最常集中在特定患者的临床特征和潜在副作用上。在对照组中,基线意向(β=0.63,p<0.01)而非PBC(β=0.04,p=0.78)预测了随访时自我报告行为中42.6%的方差。
与安大略省印刷教育信息试验结果一致,并与TPB相符,我们发现干预对任何TPB结构均无影响。该评估的理论基础为PEM干预未能改变专业行为的原因提供了可能的解释,这可为未来基于理论的改变专业行为的PEM干预的设计和内容提供直接参考。
国际标准随机对照试验编号,加拿大ISRCTN72772651。