Sunderland Geraint J, Jenkinson Michael D, Zakaria Rasheed
Department of Neurosurgery, The Walton Centre NHS Foundation Trust, Lower Lane, Fazakerley, Liverpool, L97LJ, UK.
Institute of Translational Medicine, University of Liverpool, Liverpool, UK.
J Neurooncol. 2016 Dec;130(3):535-542. doi: 10.1007/s11060-016-2254-2. Epub 2016 Sep 12.
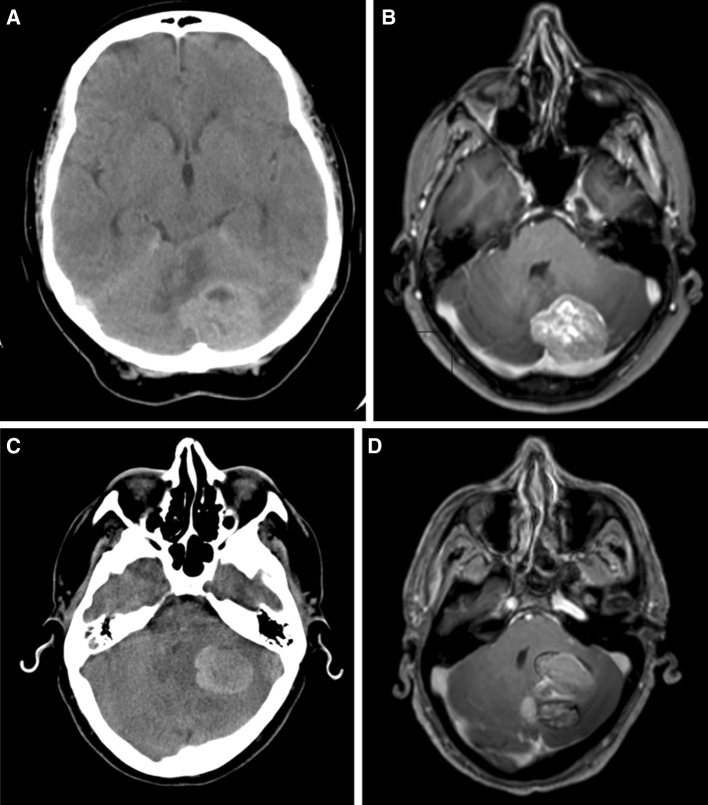
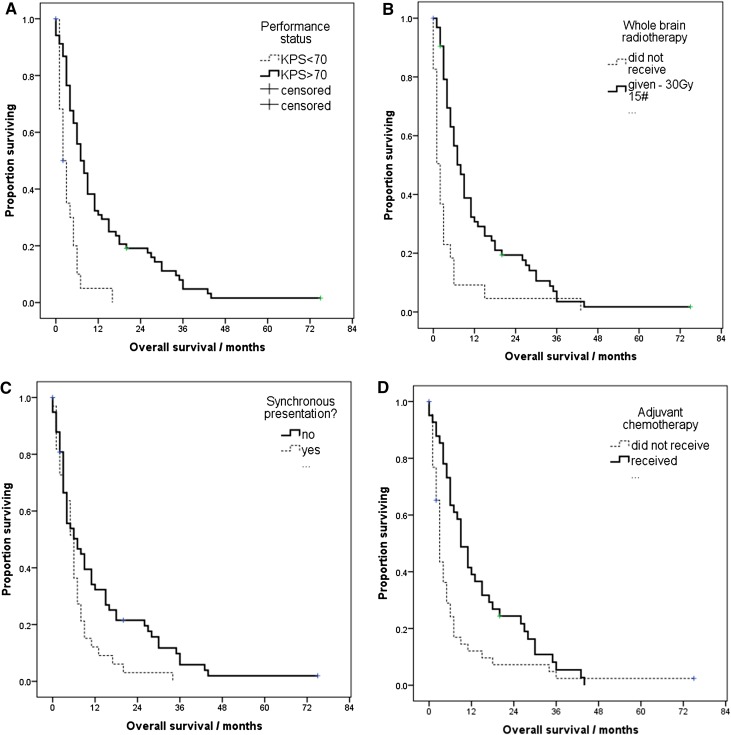
The diagnosis of brain metastases is associated with a poor prognosis reflecting uncontrolled primary disease that has spread to the relative sanctuary of the central nervous system. 20 % of brain metastases occur in the posterior fossa and are associated with significant morbidity. The risk of acute hydrocephalus and potential for sudden death means these metastases are often dealt with as emergency cases. This approach means a full pre-operative assessment and staging of underlying disease may be neglected and a proportion of patients undergo comparatively high risk surgery with little or no survival benefit. This study aimed to assess outcomes in patients to identify factors that may assist in case selection. We report a retrospective case series of 92 consecutive patients operated for posterior fossa metastases between 2007 and 2012. Routine demographic data was collected plus data on performance status, primary cancer site, details of surgery, adjuvant treatment and survival. The only independent positive prognostic factors identified on multivariate analysis were good performance status (if Karnofsky performance score >70, hazard ratio (HR) for death 0.36, 95 % confidence interval (CI) 0.18-0.69), adjuvant whole brain radiotherapy (HR 0.37, 95 % CI 0.21-0.65) and adjuvant chemotherapy where there was extracranial disease and non-synchronous presentation (HR 0.51, 95 % CI 0.31-0.82). Patients presenting with posterior fossa metastases may not be investigated as thoroughly as those with supratentorial tumours. Staging and assessment is essential however, and in the meantime emergencies related to tumour mass effect should be managed with steroids and cerebrospinal fluid diversion as required.
脑转移瘤的诊断与预后不良相关,这反映出原发疾病未得到控制并已扩散至中枢神经系统这一相对的“庇护所”。20%的脑转移瘤发生在后颅窝,且与显著的发病率相关。急性脑积水的风险和猝死的可能性意味着这些转移瘤通常作为急症处理。这种处理方式可能会忽略对潜在疾病进行全面的术前评估和分期,一部分患者接受了风险相对较高的手术,但生存获益甚微或没有生存获益。本研究旨在评估患者的预后情况,以确定可能有助于病例选择的因素。我们报告了一组回顾性病例系列,共92例在2007年至2012年间因后颅窝转移瘤接受手术的连续患者。收集了常规人口统计学数据以及关于体能状态、原发癌部位、手术细节、辅助治疗和生存情况的数据。多变量分析确定的唯一独立阳性预后因素为良好的体能状态(如果卡诺夫斯基体能评分>70,死亡风险比(HR)为0.36,95%置信区间(CI)为0.18 - 0.69)、辅助性全脑放疗(HR 0.37,95% CI 0.21 - 0.65)以及存在颅外疾病且非同步出现时的辅助化疗(HR 0.51,95% CI 0.31 - 0.82)。出现后颅窝转移瘤的患者可能不像幕上肿瘤患者那样接受全面的检查。然而,分期和评估至关重要,与此同时,与肿瘤占位效应相关的急症应根据需要使用类固醇和脑脊液分流进行处理。