Njei Basile, McCarty Thomas R, Laine Loren
Section of Digestive Diseases, Yale School of Medicine, New Haven, Connecticut, USA.
Investigative Medicine Program, Yale Center of Clinical Investigation, New Haven, Connecticut, USA.
J Gastroenterol Hepatol. 2017 Apr;32(4):852-858. doi: 10.1111/jgh.13593.
Early transjugular intrahepatic portosystemic shunt (TIPS) used as preventive therapy prior to recurrent bleeding has been recommended in patients presenting with acute esophageal variceal bleeding (EVB) who are at high risk of further bleeding and death. We investigated the impact of early TIPS on outcomes of US patients hospitalized with EVB from 2000 to 2010.
The Nationwide Inpatient Sample database was queried to identify patients with EVB and decompensated cirrhosis (because early TIPS is recommended only in high-risk patients). The primary outcome was in-hospital death, and secondary outcomes included rebleeding and hepatic encephalopathy. Early preventive TIPS was defined by placement within 3 days of hospitalization for acute EVB after one session of endoscopic therapy. Rescue TIPS was defined as TIPS after two interventions for EVB.
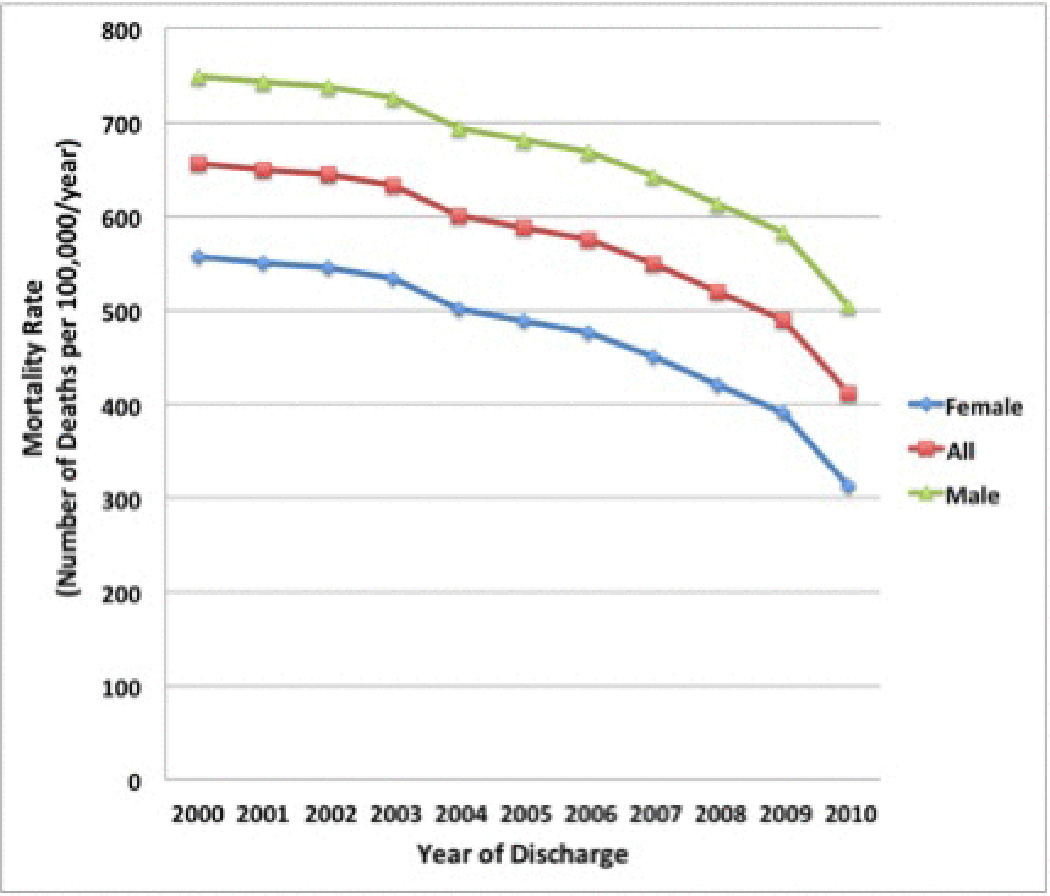
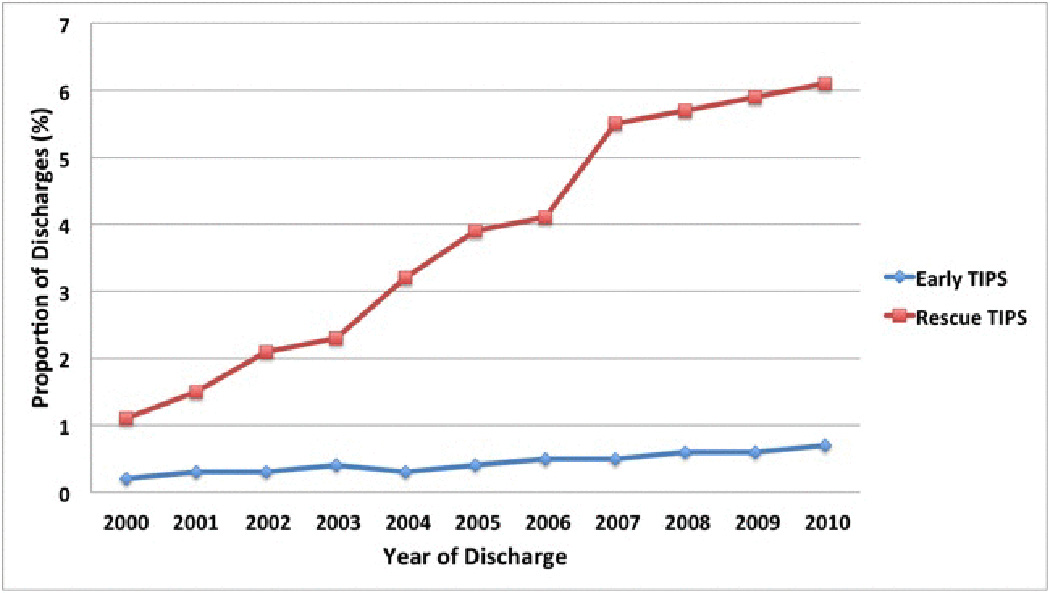
The study included 142 539 patients. From 2000 to 2010, the age-adjusted in-hospital mortality rate decreased 37.2% from 656 per 100 000 to 412 per 100 000 (P <0.01), while early and rescue TIPS increased (0.22% to 0.70%; P < 0.01 and 1.1% to 6.1%; P < 0.01). On multivariate analysis, as compared with no TIPS, early TIPS was associated with decreased inpatient mortality (risk ratio [RR] = 0.87; 95% confidence interval [CI], 0.84-0.90) and rebleeding (RR = 0.56; 95% CI, 0.45-0.71) without an increase in hepatic encephalopathy (RR = 1.01; 95% CI, 0.93-1.11).
Early preventive TIPS in patients with EVB and decompensated cirrhosis was associated with significant in-hospital reductions in rebleeding and mortality without a significant increase in encephalopathy in "real-world" US clinical practice.
对于有再次出血高风险及死亡风险的急性食管静脉曲张出血(EVB)患者,推荐早期经颈静脉肝内门体分流术(TIPS)作为复发性出血前的预防性治疗。我们调查了2000年至2010年期间早期TIPS对美国住院EVB患者预后的影响。
查询全国住院患者样本数据库,以确定EVB和失代偿期肝硬化患者(因为仅在高危患者中推荐早期TIPS)。主要结局是住院死亡,次要结局包括再出血和肝性脑病。早期预防性TIPS定义为在急性EVB住院3天内,经一次内镜治疗后进行TIPS置管。挽救性TIPS定义为在对EVB进行两次干预后进行TIPS。
该研究纳入了142539例患者。从2000年到2010年,年龄调整后的住院死亡率从每10万人656例下降了37.2%,至每10万人412例(P<0.01),而早期和挽救性TIPS的使用有所增加(从0.22%增至0.70%;P<0.01,从1.1%增至6.1%;P<0.01)。多因素分析显示,与未进行TIPS相比,早期TIPS与住院死亡率降低(风险比[RR]=0.87;95%置信区间[CI],0.84-0.90)和再出血减少(RR=0.56;95%CI,0.45-0.71)相关,且肝性脑病未增加(RR=1.01;95%CI,0.93-1.11)。
在“真实世界”的美国临床实践中,对EVB和失代偿期肝硬化患者进行早期预防性TIPS与住院期间再出血和死亡率显著降低相关,且脑病无显著增加。