Moucheraud Corrina, Owen Helen, Singh Neha S, Ng Courtney Kuonin, Requejo Jennifer, Lawn Joy E, Berman Peter
University of California Fielding School of Public Health, Los Angeles, CA, 90095, USA.
Centre for Maternal, Adolescent, Reproductive & Child Health, London School of Hygiene & Tropical Medicine, London, WC1E 7HT, UK.
BMC Public Health. 2016 Sep 12;16 Suppl 2(Suppl 2):794. doi: 10.1186/s12889-016-3401-6.
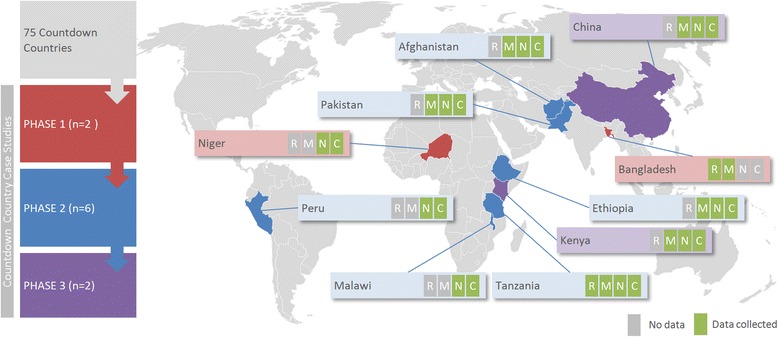
Countdown to 2015 was a multi-institution consortium tracking progress towards Millennium Development Goals (MDGs) 4 and 5. Case studies to explore factors contributing to progress (or lack of progress) in reproductive, maternal, newborn and child health (RMNCH) were undertaken in: Afghanistan, Bangladesh, China, Ethiopia, Kenya, Malawi, Niger, Pakistan, Peru, and Tanzania. This paper aims to identify cross-cutting themes on how and why these countries achieved or did not achieve MDG progress.
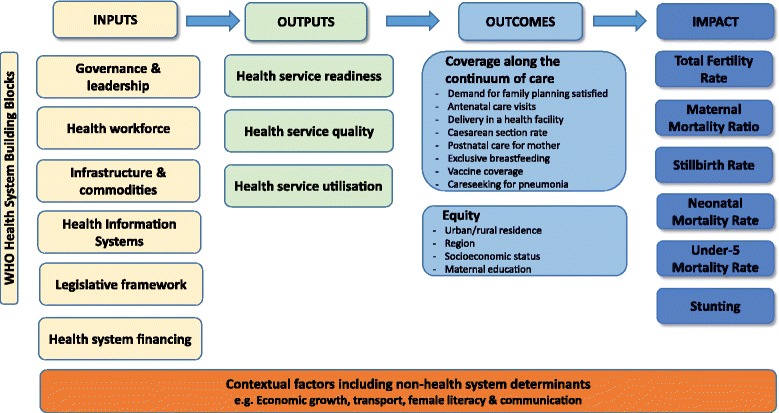
Applying a standard evaluation framework, analyses of impact, coverage and equity were undertaken, including a mixed methods analysis of how these were influenced by national context and coverage determinants (including health systems, policies and financing).
The majority (7/10) of case study countries met MDG-4 with over two-thirds reduction in child mortality, but none met MDG-5a for 75 % reduction in maternal mortality, although six countries achieved >75 % of this target. None achieved MDG-5b regarding reproductive health. Rates of reduction in neonatal mortality were half or less that for post-neonatal child mortality. Coverage increased most for interventions administered at lower levels of the health system (e.g., immunisation, insecticide treated nets), and these experienced substantial political and financial support. These interventions were associated with ~30-40 % of child lives saved in 2012 compared to 2000, in Ethiopia, Malawi, Peru and Tanzania. Intrapartum care for mothers and newborns -- which require higher-level health workers, more infrastructure, and increased community engagement -- showed variable increases in coverage, and persistent equity gaps. Countries have explored different approaches to address these problems, including shifting interventions to the community setting and tasks to lower-level health workers.
These Countdown case studies underline the importance of consistent national investment and global attention for achieving improvements in RMNCH. Interventions with major global investments achieved higher levels of coverage, reduced equity gaps and improvements in associated health outcomes. Given many competing priorities for the Sustainable Development Goals era, it is essential to maintain attention to the unfinished RMNCH agenda, particularly health systems improvements for maternal and neonatal outcomes where progress has been slower, and to invest in data collection for monitoring progress and for rigorous analyses of how progress is achieved in different contexts.
“2015倒计时”是一个多机构联盟,旨在追踪千年发展目标4和5的进展情况。在阿富汗、孟加拉国、中国、埃塞俄比亚、肯尼亚、马拉维、尼日尔、巴基斯坦、秘鲁和坦桑尼亚开展了案例研究,以探讨影响生殖、孕产妇、新生儿和儿童健康(RMNCH)取得进展(或未取得进展)的因素。本文旨在确定关于这些国家如何以及为何实现或未实现千年发展目标进展情况的贯穿各领域的主题。
应用标准评估框架,对影响、覆盖范围和公平性进行分析,包括对这些方面如何受到国家背景和覆盖范围决定因素(包括卫生系统、政策和筹资)影响的混合方法分析。
大多数(7/10)案例研究国家实现了千年发展目标4,儿童死亡率降低了三分之二以上,但没有一个国家实现千年发展目标5a(将孕产妇死亡率降低75%),尽管有六个国家实现了该目标的75%以上。在生殖健康方面,没有一个国家实现千年发展目标5b。新生儿死亡率的下降速度仅为新生儿期后儿童死亡率下降速度的一半或更低。在卫生系统较低层级实施的干预措施(如免疫接种、经杀虫剂处理的蚊帐)覆盖范围增加最多,并且这些措施获得了大量政治和财政支持。与2000年相比,在埃塞俄比亚、马拉维、秘鲁和坦桑尼亚,2012年这些干预措施挽救了约30%-40%的儿童生命。对母亲和新生儿的产时护理——这需要更高级别的卫生工作者、更多基础设施以及更强的社区参与——覆盖范围的增长情况不一,且公平性差距依然存在。各国探索了不同方法来解决这些问题,包括将干预措施转移到社区层面以及将任务交给较低层级的卫生工作者。
这些“倒计时”案例研究强调了国家持续投资和全球关注对于实现RMNCH改善的重要性。获得大量全球投资的干预措施实现了更高的覆盖水平,缩小了公平性差距,并改善了相关健康结果。鉴于可持续发展目标时代存在许多相互竞争的优先事项,必须持续关注RMNCH未完成的议程,特别是在孕产妇和新生儿结局方面进展较慢的卫生系统改进,并投资于数据收集,以监测进展情况并严格分析在不同背景下如何取得进展。