Singh Neha S, Huicho Luis, Afnan-Holmes Hoviyeh, John Theopista, Moran Allisyn C, Colbourn Tim, Grundy Chris, Matthews Zoe, Maliqi Blerta, Mathai Matthews, Daelmans Bernadette, Requejo Jennifer, Lawn Joy E
Centre for Maternal, Adolescent, Reproductive and Child Health, London School of Hygiene & Tropical Medicine, London, WC1E 7HT, UK.
Centro de Investigación para el Desarrollo Integral y Sostenible, Universidad Peruana Cayetano Heredia, Lima, Peru.
BMC Public Health. 2016 Sep 12;16 Suppl 2(Suppl 2):790. doi: 10.1186/s12889-016-3402-5.
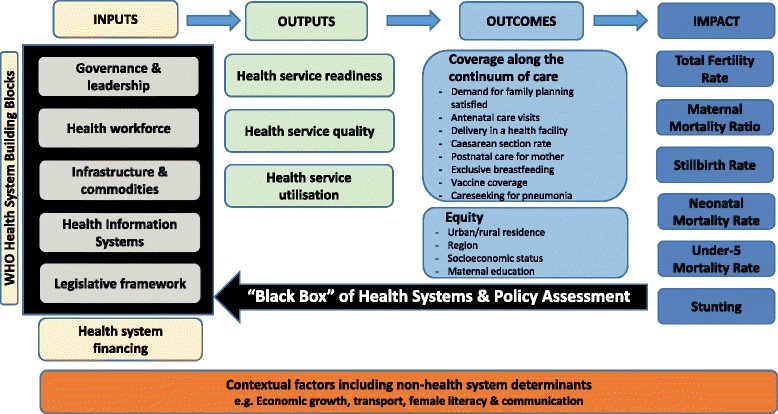
Evaluating health systems and policy (HSP) change and implementation is critical in understanding reproductive, maternal, newborn and child health (RMNCH) progress within and across countries. Whilst data for health outcomes, coverage and equity have advanced in the last decade, comparable analyses of HSP changes are lacking. We present a set of novel tools developed by Countdown to 2015 (Countdown) to systematically analyse and describe HSP change for RMNCH indicators, enabling multi-country comparisons.
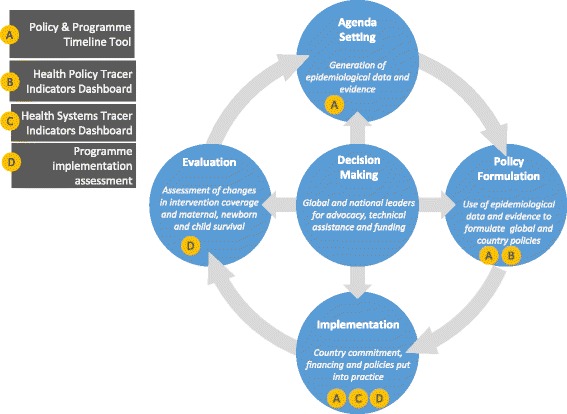
International experts worked with eight country teams to develop HSP tools via mixed methods. These tools assess RMNCH change over time (e.g. 1990-2015) and include: (i) Policy and Programme Timeline Tool (depicting change according to level of policy); (ii) Health Policy Tracer Indicators Dashboard (showing 11 selected RMNCH policies over time); (iii) Health Systems Tracer Indicators Dashboard (showing four selected systems indicators over time); and (iv) Programme implementation assessment. To illustrate these tools, we present results from Tanzania and Peru, two of eight Countdown case studies.
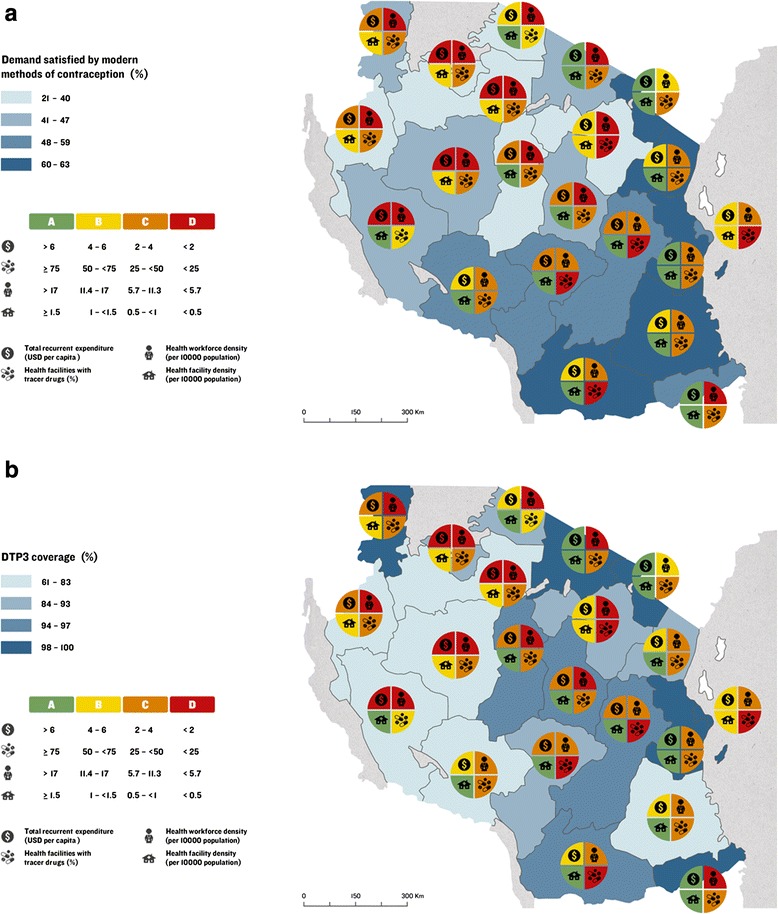
The Policy and Programme Timeline tool shows that Tanzania's RMNCH environment is complex, with increased funding and programmes for child survival, particularly primary-care implementation. Maternal health was prioritised since mid-1990s, yet with variable programme implementation, mainly targeting facilities. Newborn health only received attention since 2005, yet is rapidly scaling-up interventions at facility- and community-levels. Reproductive health lost momentum, with re-investment since 2010. Contrastingly, Peru moved from standalone to integrated RMNCH programme implementation, combined with multi-sectoral, anti-poverty strategies. The HSP Tracer Indicators Dashboards show that Peru has adopted nine of 11 policy tracer indicators and Tanzania has adopted seven. Peru costed national RMNCH plans pre-2000, whereas Tanzania developed a national RMNCH plan in 2006 but only costed the reproductive health component. Both countries included all lifesaving RMNCH commodities on their essential medicines lists. Peru has twice the health worker density of Tanzania (15.4 vs. 7.1/10,000 population, respectively), although both are below the 22.8 WHO minimum threshold.
These are the first HSP tools using mixed methods to systematically analyse and describe RMNCH changes within and across countries, important in informing accelerated progress for ending preventable maternal, newborn and child mortality in the post-2015 era.
评估卫生系统与政策(HSP)的变化及实施情况对于理解各国国内及跨国的生殖、孕产妇、新生儿和儿童健康(RMNCH)进展至关重要。尽管过去十年中健康结果、覆盖范围和公平性方面的数据有所进步,但仍缺乏对HSP变化的可比分析。我们展示了一套由“2015年倒计时”(Countdown)开发的新颖工具,用于系统分析和描述RMNCH指标的HSP变化,从而实现多国比较。
国际专家与八个国家团队合作,通过混合方法开发HSP工具。这些工具评估RMNCH随时间的变化(例如1990 - 2015年),包括:(i)政策与计划时间表工具(根据政策级别描绘变化);(ii)卫生政策追踪指标仪表盘(展示11项选定的RMNCH政策随时间的变化);(iii)卫生系统追踪指标仪表盘(展示4项选定的系统指标随时间的变化);以及(iv)计划实施评估。为说明这些工具,我们展示了八个Countdown案例研究中的两个——坦桑尼亚和秘鲁的结果。
政策与计划时间表工具显示,坦桑尼亚RMNCH环境复杂,用于儿童生存的资金和计划增加,尤其是初级保健的实施。自20世纪90年代中期以来,孕产妇健康被列为优先事项,但计划实施情况参差不齐,主要针对医疗机构。新生儿健康自2005年才受到关注,但正在迅速扩大设施和社区层面的干预措施。生殖健康失去了发展势头,自2010年起重新投入资金。相比之下,秘鲁从独立的RMNCH计划实施转向综合实施,并结合了多部门的扶贫战略。HSP追踪指标仪表盘显示,秘鲁采用了11项政策追踪指标中的9项,坦桑尼亚采用了7项。秘鲁在2000年前对国家RMNCH计划进行了成本核算,而坦桑尼亚在2006年制定了国家RMNCH计划,但仅对生殖健康部分进行了成本核算。两国在基本药物清单中都列入了所有挽救生命的RMNCH商品。秘鲁的卫生工作者密度是坦桑尼亚的两倍(分别为每万人口中15.4人和7.1人),尽管两国均低于世界卫生组织规定的22.8 的最低阈值。
这些是首批使用混合方法系统分析和描述各国国内及跨国RMNCH变化的HSP工具,对于为在2015年后时代加速实现消除可预防的孕产妇、新生儿和儿童死亡的进展提供信息至关重要。